




Malpractice insurance is not built for the new healthcare order
Get Out-Of-Pocket in your email
Looking to hire the best talent in healthcare? Check out the OOP Talent Collective - where vetted candidates are looking for their next gig. Learn more here or check it out yourself.
 Hire from the Out-Of-Pocket talent collective
Hire from the Out-Of-Pocket talent collectiveFHIR 101

Featured Jobs
Finance Associate - Spark Advisors
- Spark Advisors helps seniors enroll in Medicare and understand their benefits by monitoring coverage, figuring out the right benefits, and deal with insurance issues. They're hiring a finance associate.
- firsthand is building technology and services to dramatically change the lives of those with serious mental illness who have fallen through the gaps in the safety net. They are hiring a data engineer to build first of its kind infrastructure to empower their peer-led care team.
- J2 Health brings together best in class data and purpose built software to enable healthcare organizations to optimize provider network performance. They're hiring a data scientist.
Looking for a job in health tech? Check out the other awesome healthcare jobs on the job board + give your preferences to get alerted to new postings.
This episode of Out-Of-Pocket is brought to you by…
Most practices overpay for malpractice insurance because they don’t have time to shop. With Docshield, you can apply for quotes in 15 minutes and compare coverage options side by side from A-rated national insurers including The Doctors Company, MedPro, Coverys, and ProAssurance.
See what you should be paying at docshield.com.
–
Law Suit and Tie Sh**
We absolutely love suing in the US. We even send the kids to mock trial just to microdose the experience.
That lawsuit culture bleeds into healthcare when it comes to malpractice suits. We’re an extremely litigious country when it comes to suing doctors, and as a result it yields all kinds of downstream effects in medicine. Extra tests are ordered, things are done just to cover yourself in a lawsuit, it becomes a plotline in the Pitt, and doctors have to deeply think about the kind of malpractice coverage to get.
Malpractice insurance has largely stayed stagnant, but I think two factors are going to impact it: AI and a fracturing standard of care. This is going to require new muscles from malpractice carriers, and potentially new products.
Today we’re going to be talking about how malpractice works, and how new practices that deviate from the standard of care (e.g. longevity companies) are introducing new questions around malpractice. Next time we’ll talk about the AI piece.

{{interlude 3}}
How does malpractice insurance work
Because malpractice suits can result in massive financial judgments, most physicians carry malpractice insurance to cover legal defense and any damages awarded.
Malpractice awards look at damages in two buckets: Economic damages (medical bills, lost income, direct costs) and noneconomic damages (pain and suffering, loss of quality of life). But state damage caps put a ceiling on the noneconomic bucket - twenty-nine states currently have some form of cap still standing. In states without caps the verdicts can become very large, e.g. $200M with $80M coming from non-economic damages.
The tradeoff states make is whether you think patient outcomes get worse without malpractice risk and whether capping non-economic damages harm lower-income people more.
There are different flavors of malpractice insurance.
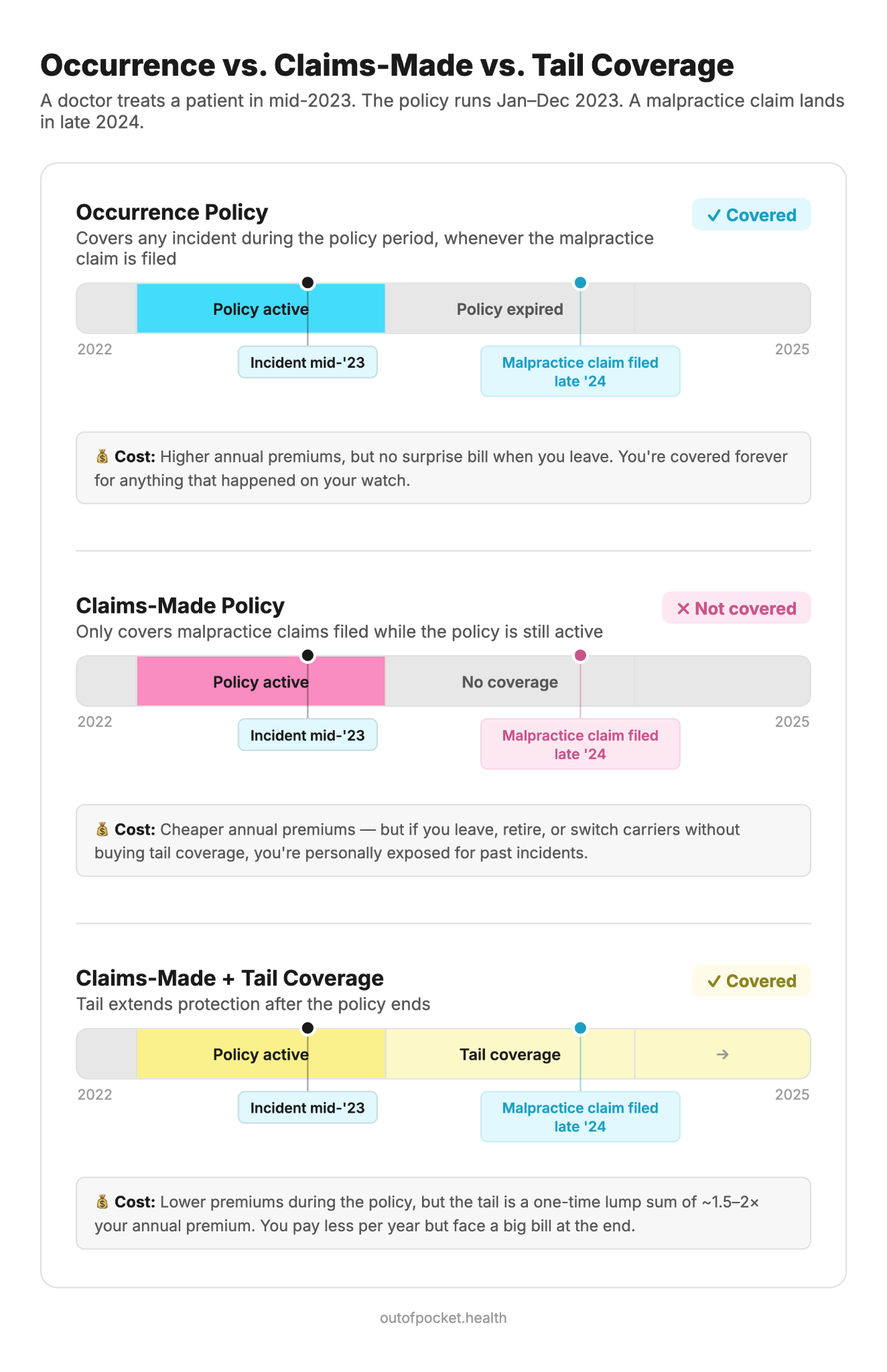
- Occurrence - You can get coverage that covers the time period when a patient says you goofed. This will cover you whenever the claim is made, even if it’s years later.
- Claims-made - You can get just claims-made, which cover you if the claim is made while the policy is in effect. This is much cheaper, but can leave you with gaps.
- Tail coverage - Unrelated to furries. This is usually something you’d add on to a claims-made coverage as a lump sum payment to protect you after your policy lapses. This is typically used to cover you as you’re switching jobs, insurance carriers, or sliding into retirement and want peace of mind.
- Nose coverage - You’d get this to cover incidents that happen before a NEW policy gets started. If a doc changes jobs, the new employer might cover nose coverage for cases at your current job (if you don’t have your own coverage).
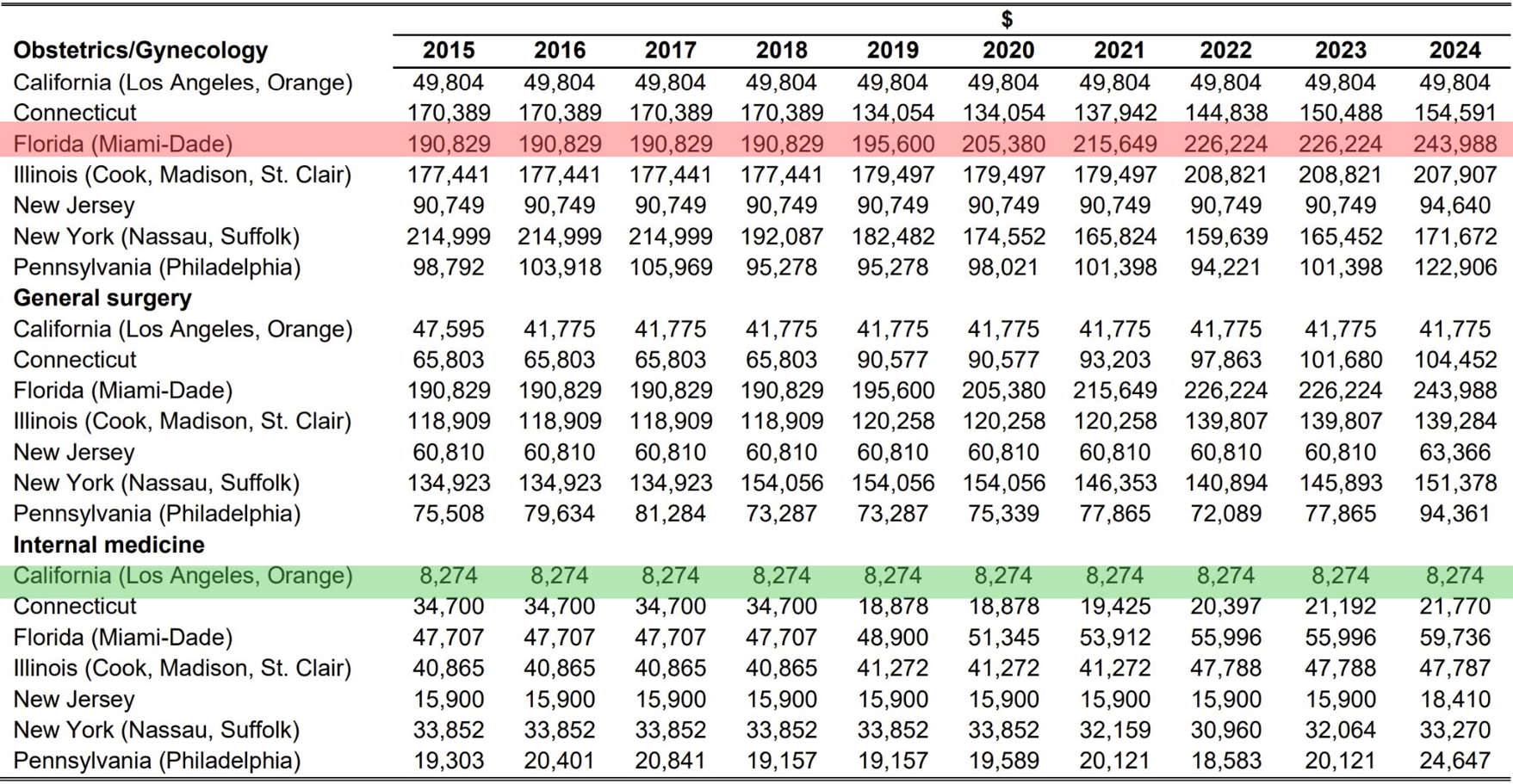
The cost of malpractice insurance varies enormously. An internal medicine physician in California might pay $8,000 a year, while an OB/GYN in Miami-Dade paid nearly $244,000 for the same policy limits in 2024. Three factors drive most of the variation:
- Specialty: Surgeons and OB/GYNs consistently pay 3–5x what primary care physicians pay, reflecting higher procedural risk and larger average verdicts.
- Geography: Florida, New York, and Illinois are the most expensive states, driven by high claim frequency and large jury awards. States with caps on noneconomic payouts have lower premiums.
- Claims history: If you have high payouts in the past, your premiums are going to be higher for your policies.
As you can imagine, this becomes a barrier for physicians starting a practice. Procedures bring in the money but also present more risk for malpractice. A neurosurgeon or OB/GYN in a high-premium state is looking at six figures in insurance costs before seeing a single patient. When you join a large health system, the institution carries the coverage, pools risk across all its physicians, and absorbs most of the legal exposure.
[I’d be curious from physicians reading this how malpractice ranks on your reasons for not being independent vs. things like getting patients, upfront costs, looking down on peers from the ivory tower of an academic medical center, etc.]
Who actually decides what “standard of care” means?
A core aspect to malpractice suits is figuring out whether or not a physician did the “standard of care”. As Dr. Eric Funk told us in an interview in 2021 Out-Of-Pocket (throwbackkk)
“Theoretically, the doctor is judged by the "standard of care". The legal definition of the standard of care is nuanced and widely debated, but basically boils down to what a reasonable doctor would have done in a given situation. If no responsible doctor could have made the diagnosis or prevented the bad medical outcome, then the doctor should not have a legal judgment decided against them.
However, the reality of medical malpractice trials is much more complicated. If the lawsuit goes all the way to trial, the physician is going to be judged by 12 people with no medical training. These cases are often medically complicated and require high levels of expertise to understand, but in the end, 12 average citizens will decide if the doctor was "right" or "wrong". - Dr. Eric Funk
When a malpractice case gets evaluated expert witnesses play a core role in how that concept of standard of care gets decided. One says the test should have been ordered sooner. The other says the symptoms didn’t warrant it. Interrater reliability rears its ugly head again.
The "standard of care" is basically whatever they can convince a jury of. This concept is important and changing quite a bit now.
Out-Of-Pocket is also supported by…

When patients leave the standard of care + continuous monitoring
Right now many people are dissatisfied with “the standard of care”. In fact, they are willing to pay more money specifically to have a doctor explore areas where there isn’t a standard of care. Concierge clinics are an example of this.
But when there is no real standard of care, it becomes harder to figure out what malpractice actually looks like. Many concierge clinics are getting priced as standard primary care because that’s the doc’s specialty on paper. But because of the way they practice, the actual risk profile is totally different. Some longevity/concierge specific malpractice products seem to be emerging.
One particularly interesting side of these clinics is continuous monitoring and testing people while healthy. This sounds really attractive to patients, if you get more tests you’ll catch more things! But on the flipside, testing more also means that you’ll naturally catch more anomalous issues that might not be worth bringing up or miss more that you were expected to catch. This increases the surface area of malpractice suits.
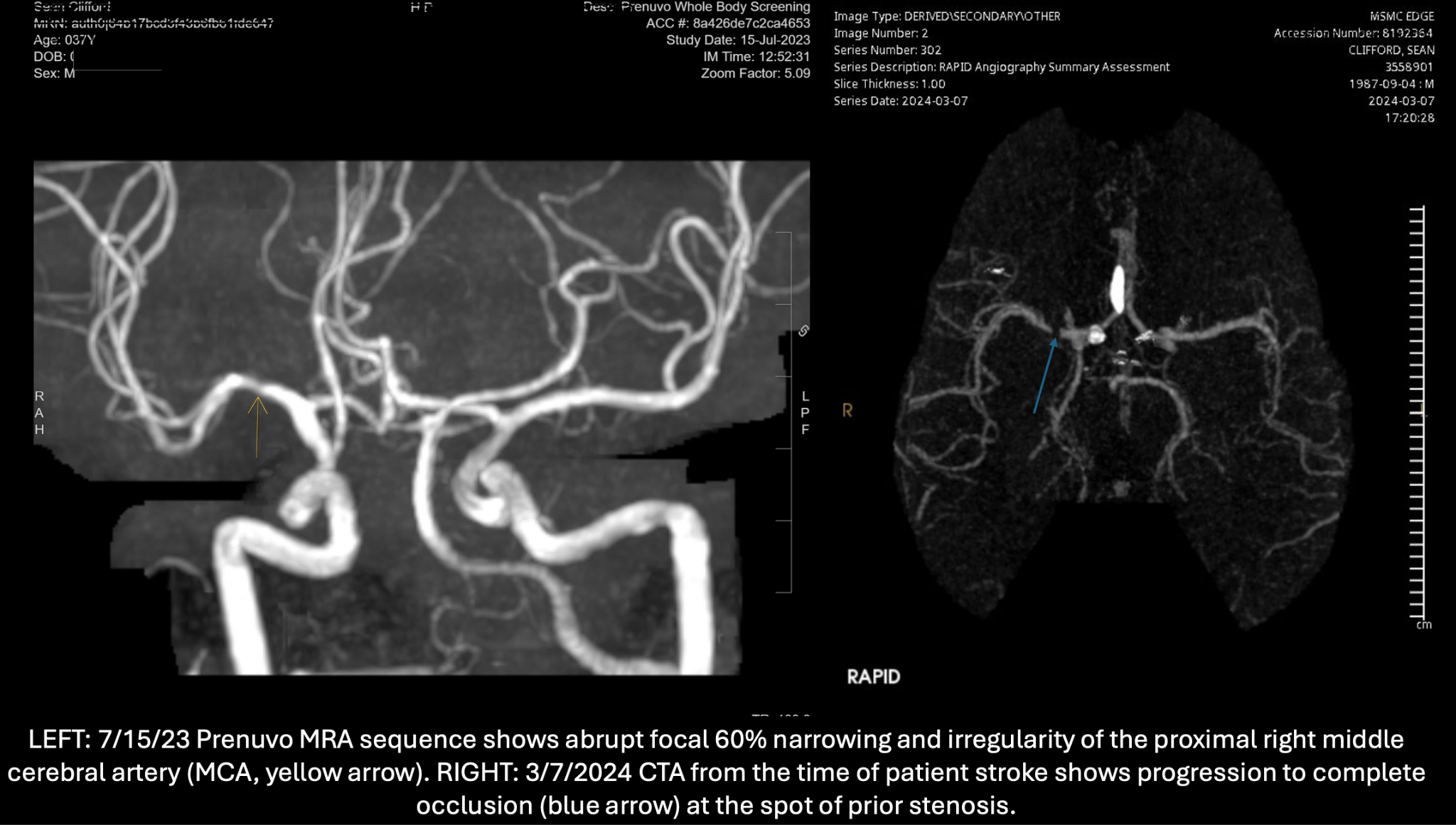
We’re seeing this play out in some areas like this Prenuvo malpractice suit. A 37-year-old with no risk factors gets an elective whole-body MRI. The AI-assisted scan came back clean but eight months later he had a catastrophic stroke. The lawsuit alleges the radiologist missed a 60% stenosis that was visible on the scan. When you increase the volume of scans you do, you’re naturally going to get way more of these misses.
You can bring this argument to areas like regular lab testing or even wearables that are now giving you indications about your health. If a new practice integrates wearables into their clinic, are they expected to provide guidance for every datapoint under the risk of malpractice? Do they need to reach out every time my heart rate spikes when my fat ass finally goes to a cardio class which is so rare that it’s flagged as an anomaly?
A malpractice policy will probably have to take that into account. The malpractice coverage is structured as “when something occurred” for occurence/claims-made policies and thinks about care as a specific episode. But if you’re continuously monitoring, when does something count as an occurrence?
Or what about using different intervention choices? For example using a more aggressive statin protocol, a GLP-1 for someone who doesn’t technically qualify, sus peptides, whatever Bryan Johnson is putting in his taint. Sure in some ways patients are paying into this and specifically being told that this is what they’re getting - but how far does informed consent actually go here?
I wonder whether in the future, the doctor in a malpractice case at one of these clinics is compared against what a regular primary care doc would do in that situation, a longevity doctor specifically, or against a specific “longevity protocol”.
Conclusion - the shift continues
We’re at an interesting juncture where the gap between “interesting research” and “becomes a part of the standard of care” is getting wider.
As more research comes out and is easier to access/analyze with AI tools - people are going to want more of this, physicians are going to try new things, and more lawsuits are going to happen when it comes to the standard of care.
Shifts to the standard of care aren’t new and we have frameworks to think about this. But that’s not necessarily true when it comes to how AI tools are used in practices. In the next episode, we’re going to talk about how AI is going to force malpractice carriers to rethink their underwriting and processes. Sign up to get it.
Thinkboi out,
Nikhil aka. “Malpractice? Talking about Malpractice? Not the game, but malpractice”
P.S. Last call to sign up for our free AI x RCM masterclass, especially useful if you’re a mid-size specialty group (who probably feels the pain of these malpractice woes I’m talking about)
This was written with help from Lauren Risenhoover. Thanks to Aqil Rashid and Dr. Eric Funk for reading drafts.
Twitter: @nikillinit
Other posts: outofpocket.health/posts
{{sub-form}}
If you're enjoying the newsletter, do me a solid and shoot this over to a friend or healthcare slack channel and tell them to sign up. The line between unemployment and founder of a startup is traction and whether your parents believe you have a job.
Quick Interlude - NEW COURSE ON FHIR! KNOWLEDGEFEST APPS DUE SOON!
See All Courses →So...what actually is FHIR? I get this question a lot, but there's never really enough time to explain it and also I would just mumble "technical standard" and walk away.
So we decided to do a standalone free FHIR 101 course in partnership with Redox! Over 3 days in August we'll go over the spec itself, how it differs from other healthcare information standards, and practical tips to build with it.
I wanted to call it FHIR fest but it got nixed. You can sign up for it here, it's FREE and it's 8/25-8/27.

And a reminder that Knowledgefest apps are due this week. If you want to be in a room with the best ops people in healthcare, you should apply like TODAY.
We sell this conference out every year - all workshops, learn how people are building and scaling in healthcare, application based so we only take the best. We have people from Commure, Clarity Pediatrics, Pomelo, and Waymark already coming, join the squad.

Get Out-Of-Pocket in your email


