




Wearables have some issues to fix
Get Out-Of-Pocket in your email
Looking to hire the best talent in healthcare? Check out the OOP Talent Collective - where vetted candidates are looking for their next gig. Learn more here or check it out yourself.
 Hire from the Out-Of-Pocket talent collective
Hire from the Out-Of-Pocket talent collectiveHealthcare 101 Crash Course
%2520(1).gif)
Featured Jobs
Finance Associate - Spark Advisors
- Spark Advisors helps seniors enroll in Medicare and understand their benefits by monitoring coverage, figuring out the right benefits, and deal with insurance issues. They're hiring a finance associate.
- firsthand is building technology and services to dramatically change the lives of those with serious mental illness who have fallen through the gaps in the safety net. They are hiring a data engineer to build first of its kind infrastructure to empower their peer-led care team.
- J2 Health brings together best in class data and purpose built software to enable healthcare organizations to optimize provider network performance. They're hiring a data scientist.
Looking for a job in health tech? Check out the other awesome healthcare jobs on the job board + give your preferences to get alerted to new postings.
Want us to make you look cool? Let’s chat, we’re good partners I promise.
Wearables, and Wear-not-ables
In Part 1, me, Afnan, and Samir talked about why it’s the time for wearables. And in Part 2 it’s “Sike I lied”.
This last weekend we spent A LOT of time with wearables at our Hardware Hackathon. Today we’ll talk about some of the areas wearables will need to overcome to reach their potential. We’ll be blending our perspectives and writing in the first person so you don’t know who to get angry at (it’s Samir, blame him).
A few areas we think wearables still need some work.
{{interlude 3}}
Onto the show
Standardization in data readouts and “new” biomarkers
Despite these advances, wearables aren't ready for widespread clinical adoption. One core problem is standardization across the data that comes out of wearables
Heart rate variability is the poster child for this problem. HRV is a popular metric that varies dramatically based on which specific metric is calculated, data quality and collection methodology, timing of measurement (rest vs. active vs. sleep), and device-specific algorithms. Without standardization, clinicians and researchers can't make consistent decisions based on wearable data. The same patient wearing two devices might get contradictory readings.
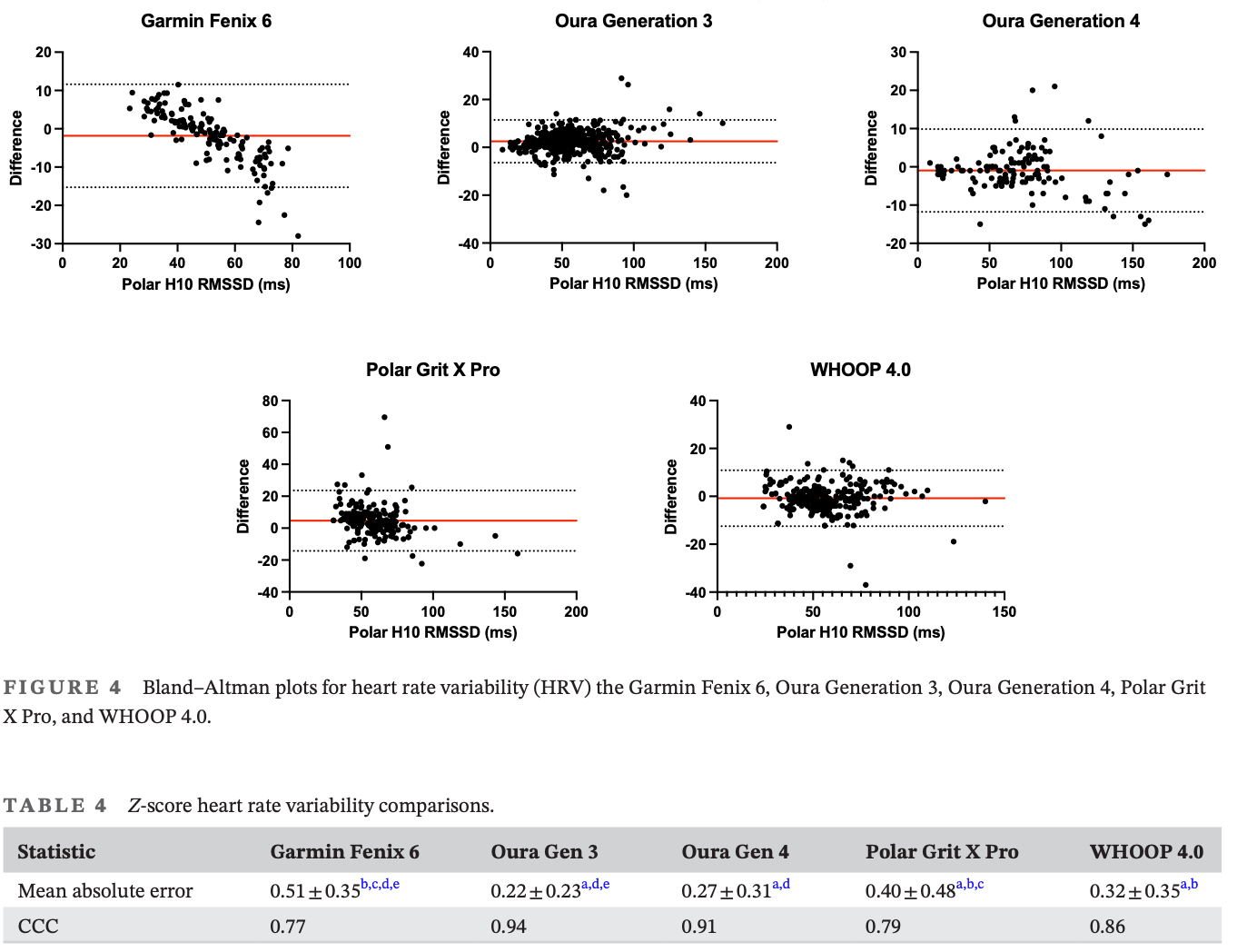
More data from more devices with more proprietary algorithms means more noise unless we establish common frameworks. And now every wearable company is now inventing its own composite scores like Recovery, Readiness, Strain, etc. They all use overlapping inputs (HRV, resting heart rate, sleep, respiratory rate) but weight them differently, measure the underlying signals differently, and slap different names on the output like Cardiovascular Age. I’ve been telling people I have a 16 year old’s heart in me and the police were called several times.
If you wanted to study these or use them in your practice, how would you know which recovery score to use or “Biological Age” score to use if they’re all different? There’s an incentive to keep those biomarkers proprietary to the company, but that’s also going to be the exact thing that makes it hard to adopt.
The adoption gap for lower income/older patients
All those wearable benefits would be nice…if they’re actually used by people who have the most to gain.
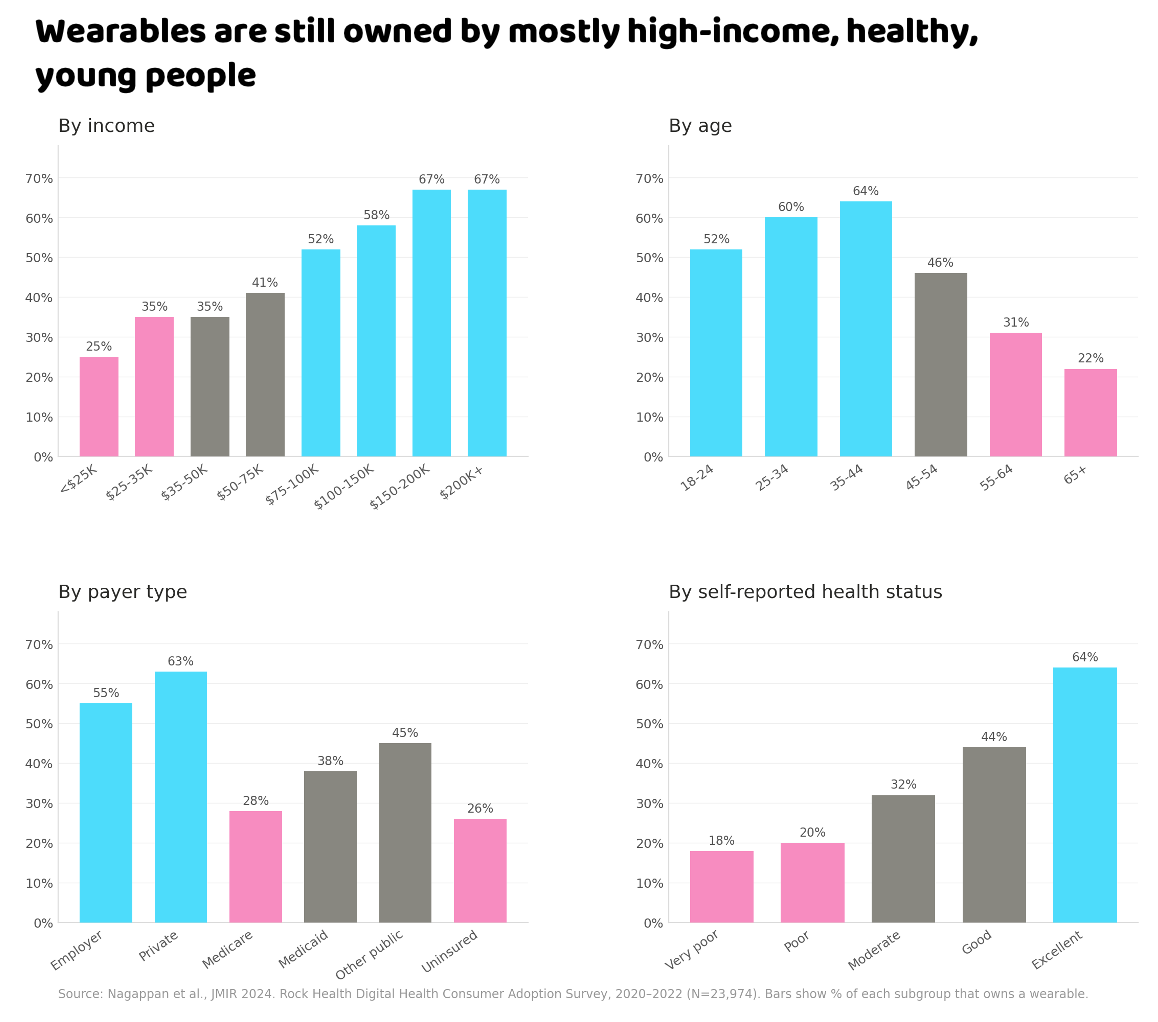
The reality right now is that wearables are still mostly used by young, healthy, affluent people. I’m in that group, and yet somehow that doesn’t feel like stunting on ‘em in this context.
The open question is how we get more people to use devices. There are a few gaps to solve.
Payment - The most obvious is that the devices are still quite expensive. One way to bridge the gap is for alternate payment mechanisms to cover it on the users behalf. For example, several Medicare Advantage plans have offered wearables to patients like Devoted Bucks, Oura <> Essence, etc. But there’s still gaps for lower income/Medicaid/uninsured patients to get their hands on this (or…get this on their hands).

User Experience/Utility - A lot of wearables are still pretty complex to get set up and have a lot of tricky user experience issues to get around. For example the need to charge them regularly, you need to pair them with a smartphone via Bluetooth, you need to navigate the companion app to actually interpret the data, wait what’s my login again?
There's a product design opportunity here: devices purpose-built for clinical populations rather than fitness enthusiasts. Longer battery life, simpler interfaces (e.g. voice AI?), automatic data sharing with care teams, and fewer features that require manual configuration. The clinical-grade RPM devices are further along in this direction and might have some user experience elements to borrow.
Distribution - You still need to get wearables into patients hands. Some of the Medicare Advantage companies can act as both payments and distribution, AARP has reward systems for connecting wearables, etc. But the missing piece IMO is clinicians recommending it themselves, which really means showing utility (and payment) to the docs.
False Positives + creating new care models and workflows
What time is it? It's. Time. To. DO SOME POPULATION HEALTH STATISTICS!!! The groans in unison emanate from the newsletter. But we need to do this math because it points out a big unsolved problem for wearables. When millions of people are tracking potential anomalies, how do you deal with the tens of thousands of false positive notifications?
The Apple Heart Study enrolled 419K people and pushed irregular rhythm notifications to their wrists. Of the people who got flagged and followed up with an ECG patch, only 34% actually had AFib. The Fitbit Heart Study did basically the same thing with 455,000 people and got roughly the same % confirmed AFib. Two out of three alerts didn’t lead to a confirmed diagnosis, and might have been an Afib that resolved itself. But those patients still got a notification you need to deal with.
AFib prevalence in your average wearable-wearing population is like 1%. When you screen millions of mostly-healthy people for something rare, even a great test produces way more false positives than true positives. This is just how the math works despite tech people not believing false positives are a real thing.
We are going to need to build entirely new workflows that can triage patients who are getting alerts. 57% of people who got ANY notification in the Apple Heart Study went to a healthcare provider about it. AI, asynchronous and telemedicine consults, guiding people to the right care in-person that can see them quickly, new forms of in-person care with tools to get more data for triaging, etc. Think of it like the urgent care for wearable anxiety - there’s even new terms popping up for this (e.g. orthosomnia for obsessive sleep trackers, “extremely single” for people that really care about their resting heart rate).
There’s also the opposite problem, a lot of people that get the notification DON’T get it triaged. In the Fitbit Heart Study, out of ~4,700 people who got an irregular heart rhythm notification, only about 1,700 even followed up with the telehealth visit, and only ~1,000 ended up with an ECG patch. That means roughly 3,000 people got a notification that basically said "hey, your heart might be doing something weird" and then just…didn’t do anything. Some of them probably had real AFib that went unconfirmed. We don't know, because they fell out of the funnel.
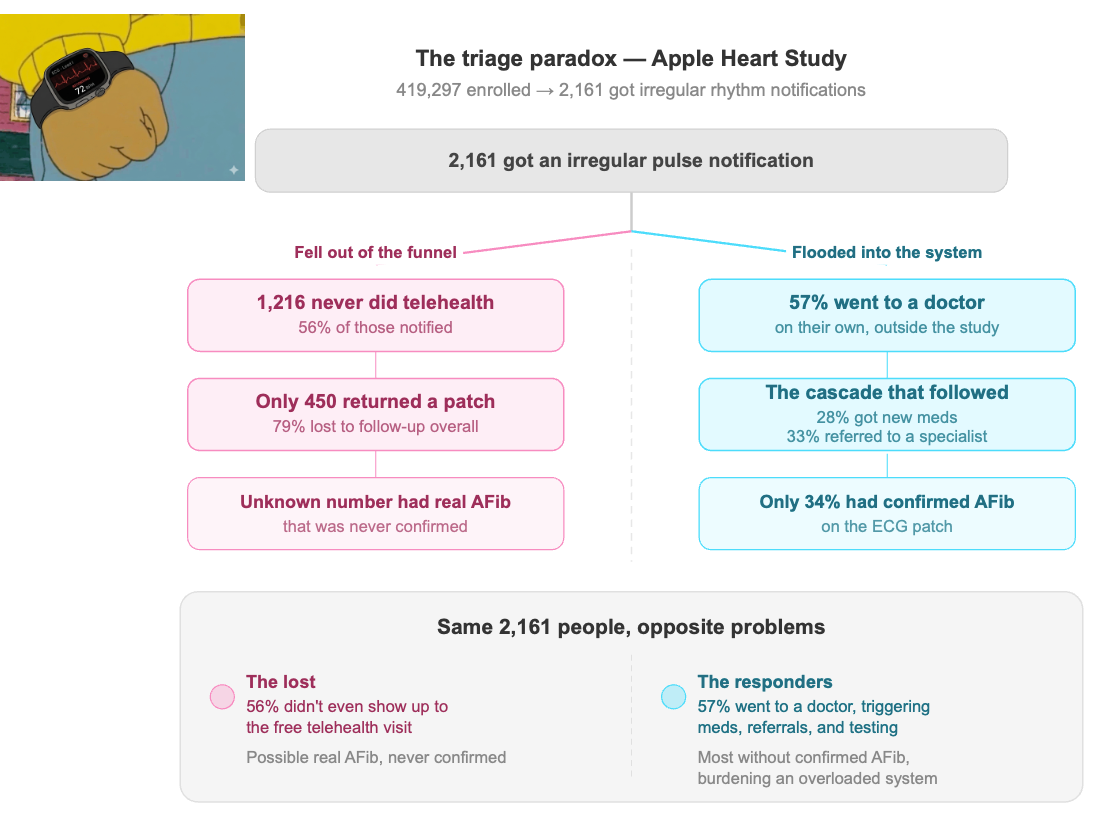
So you've got this bizarre situation where wearables are simultaneously creating a flood of worried-well people showing up to ERs AND failing to get the actually-sick people to follow through on confirmation.
This means we’re going to need better ways for providers to actually ingest data from wearables into their existing workflows to address these patients differently. Today that’s a basically non-existent bridge, but the next wave of brick-and-mortar clinics will have to figure out how data feeds from wearables are surfaced appropriately vs. treated as a distraction.
Can AI finally interpret the data?
Wearables have always captured a lot of data, but it’s been hard to get anyone to read it when there’s so much of it and a ton of noise. If you take the reams of Apple Watch data and ask your doctor to make sense of it, they want to chuck you and your Apple Watch out of the window, (“hey my heart rate stopped!”). No one has time to sift through weeks of heart rate variability trends to find the signal in the noise.
AI SHOULD provide one of the critical missing pieces - a tool that can sift through large amounts of unstructured data and actually help you make sense of it. On top of that, it can ask follow up questions + take data from other places (e.g. your EHR data) to get even more context that makes it specific to you.
However, we’re not quite there YET. LLMs give the vibe that they can help analyze the data, but in practice they can create spurious linkages that may not exist in an attempt to stitch together a story. They also might tell people exactly what they want to hear if they ask them about their wearable data vs. what is objectively true. But it’s still better than a 4 month wait to see a doctor if you think you might have an issue.
If you have a targeted question AND know you can trust the data/know what data to use, LLMs can bridge the gap to answering it. Fixing some of the issues we talked about above (standardization, etc.) can help with this, but it’s also possible you will need purpose-built applications that can interpret this data vs. general LLMs like chatGPT or Claude.
Conclusion and a story (from Afnan)
Wearables are most powerful when three things align: the signal has meaning, you can change something based on it, and someone knows how to interpret the signal in context.
Let me tell you about my mom.
She's a typical South Asian woman in her 60s - hypertension, diabetes, loves roti. Things were manageable until she developed IgA nephropathy. Then everything accelerated. Her kidney function worsened quickly. We were weeks away from dialysis. We got her listed for transplant. We had the conversation no one wants to have, where you sit at a dinner table and talk about giving your parent a kidney. We cried.
The acute phase resolved after monoclonal antibodies, but the damage remained. Diabetes and blood pressure still mattered, and her kidneys weren't recovering. So we focused on the small things.
We connected a blood-pressure cuff. We started continuous glucose monitoring. For the first time, we could see how daily life like meals, stress, sleep, and movement affected her physiology. We learned that yellow daal was fine, black daal was not. Stress mattered more than dessert. Walking for 15 minutes after dinner consistently blunted her glycemic response.
But it wasn't the device alone. She had context, human involvement, and translation to make sense of all of it. And she had agency in her care by understanding how activities in her control affected her health.
Her A1c dropped from 9.7 to 6.3 in four months. Four years later, her kidney function has stabilized. She still has flares. She has an excellent nephrologist. And she gets to walk through Disneyland with my kids.
That's what wearables can do when someone knows how to listen. We still have a lot of problems to solve (standardization, etc.). So we're not there yet, but we're closer than we've ever been.

Thinkbois out,
Nikhil, Samir, and Afnan aka. Three Headed GOAT biryani
Twitter: @nikillinit
IG: @outofpockethealth
Other posts: outofpocket.health/posts
If you’re enjoying the newsletter, do me a solid and shoot this over to a friend or healthcare slack channel and tell them to sign up. The line between unemployment and founder of a startup is traction and whether your parents believe you have a job.
Interlude - Apply to Knowledgefest! And healthcare 101 starts next week!
See All Courses →Don’t forget the application for our Knowledgefest, our healthcare software engineering conference IS LIVE.
If you work in healthcare ops, you want to be here. This is where you learn playbooks, see what other ops people are doing, and build your network. It’s year 5 and we sell out every year - applications are due end of month.
And if you feel like you really need to get up to speed on how healthcare works, then you should let me teach you at Healthcare 101starting next week!This is for anyone hiring teams of non-healthcare people that need to get up to speed quickly (in 2 weeks) - we do group discounts too hit up ya boy. You’ll even learn how to make memes.
.png)
Get Out-Of-Pocket in your email


