




(Ethically dubious) ways to give patients more choice
Get Out-Of-Pocket in your email
Looking to hire the best talent in healthcare? Check out the OOP Talent Collective - where vetted candidates are looking for their next gig. Learn more here or check it out yourself.
 Hire from the Out-Of-Pocket talent collective
Hire from the Out-Of-Pocket talent collectiveFHIR 101

Featured Jobs
Finance Associate - Spark Advisors
- Spark Advisors helps seniors enroll in Medicare and understand their benefits by monitoring coverage, figuring out the right benefits, and deal with insurance issues. They're hiring a finance associate.
- firsthand is building technology and services to dramatically change the lives of those with serious mental illness who have fallen through the gaps in the safety net. They are hiring a data engineer to build first of its kind infrastructure to empower their peer-led care team.
- J2 Health brings together best in class data and purpose built software to enable healthcare organizations to optimize provider network performance. They're hiring a data scientist.
Looking for a job in health tech? Check out the other awesome healthcare jobs on the job board + give your preferences to get alerted to new postings.
Oh you like consumerism? Name every buyable experience
Everyone likes to say they want to make healthcare more of a consumer experience. But how far do they want to take that? How far should we take consumerism? Everyone is pro-consumerism until I suggest a marketplace for organs.
A few years ago we talked about ways to empower patients with things like class action lawsuits, data ownership, etc. But today I’d like to do a few thought experiments on even MORE out there (and largely illegal) ways we can give patients options at the extreme level. Let’s see how comfortable people are with these ideas.
Most of these thought experiments are not possible in the way we’ve structured US healthcare today, but have analogs that are legal outside of healthcare or in other countries. These scenarios are meant to push you in how you think about the tradeoffs we make between quality, patient safety, choice, etc.
Below are some of my more out there ideas on how we could give patients more choice and take on more liability.
Patient could trade data for services
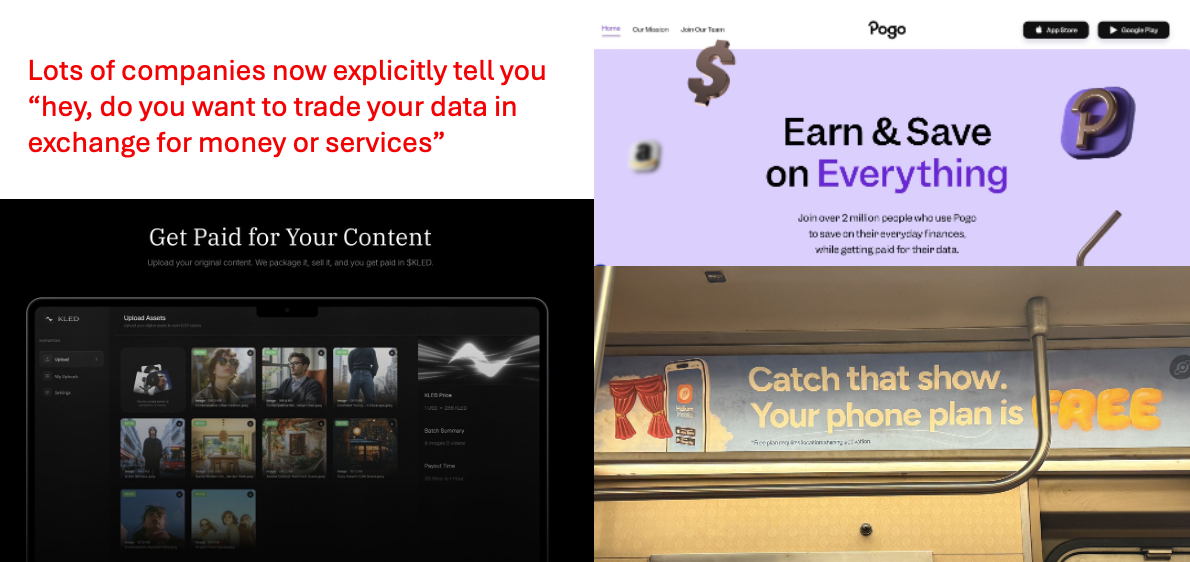
One trend I’ve been seeing outside of healthcare are companies that explicitly say “hey, give us your data. In exchange we’ll give you money or a service for free”.
This has been happening implicitly for a while - e.g. Facebook and Google are free because they use your data to serve you personalized ads. But this next wave of companies take it to a different level, where they say “hey upload your photos or your receipts and we’ll give you money for that”. It’s a much more explicit exchange for first-party data they can’t access easily just from your usage of the platform.
I would guess this is happening for a few reasons:
- Everything is more expensive, so people are willing to do anything for money. I’ve done worse for less.
- People feel like their data is already being monetized or is out there already, so they might as well get a cut of it.
- Companies are willing to pay for first-party data because it’s cleaner and they can get follow up data directly from users (e.g. follow up surveys if a user meets certain criteria, or ask those users to stitch other datasets together that might be relevant).
This is also true in healthcare - we’ve talked in the past about how data brokers work for patient data and why we’re starting to see a push for first-party data. In the age of AI models wanting increasingly more (hard to access) healthcare data, this seems to be even more true.
So here’s my idea…what if you could choose whether you got subsidized healthcare services, but in exchange your data was sold? You have a choice: your specialist visit is either going to be a $50 co-pay or $20 if we can package all of your data (not just healthcare), sell it, and you have to fill out a survey for extra data.
This is kind of a gray area in medicine and is generally viewed as potentially inducement and/or violating Stark/Anti-kickback laws.
But there are lots of reasons this might not work even aside from the ethical and legal ones. The individual’s data is not that valuable and already relatively accessible today for commercial purposes so you can’t really reduce the price by that much. Maybe you do something else non-monetarily like let people who opt-in to data sharing get appointments faster.

{{interlude 3}}
Make my healthcare case an exhibition
I read an interesting story about Martin Couney. He basically wanted to test if chicken incubators could be used for premature babies. In order to cover the cost, he made it a part of carnivals to see this being done. Turns out it worked extremely well, though many docs considered him a “tasteless showman” (today, would be called a cringe merchant).

There weren’t many places that could take care of premature babies at the time, and even then it was considered extremely expensive. This exhibition used the public’s fascination to fund it, not charge patients, and make Couney himself wealthy. It also was then able to prove the incubator actually worked to help the children, essentially funding the R&D costs as well.
Maybe more of medicine should be an exhibition. Anyone who’s been in a hospital knows how absolutely sick medical technology is. Surgery amphitheaters used to be open to the public, and doctors would narrate what was happening while it happened. The success of the Pitt makes me think medical voyeurism is an untapped market.
So here’s my weird idea - if you consent to allowing the public to watch your surgery, you don’t have to pay anything in co-pays, co-insurance, etc. The surgery would be ticketed, and the cost of those tickets would cover it instead. Or have a Twitch livestream of your therapy session, and the ad revenue covers the cost of the service for you (which already kind of exists).
Obviously extremely weird and ethically dubious for lots of reasons. Will only people that can’t afford it take the option? Would you do things during the surgery to “satisfy viewers” that wouldn’t be done normally? Would people actually be dissuaded from doing surgery if they see a complication?
But there might be some benefits!
- Patients that can’t afford a service have an alternate means of getting it paid for
- More of the public gets exposed to technology/events that are typically isolated in the hospital setting. That might make them more interested in medical technology, more trusting of docs if they see what they do, etc.
- People get to see other patients, and potentially find out they might have an issue by seeing a different patient get treated.
- Individual doctors can build their reputation, following, and trust with the public by showing what they do.
Let’s make a healthcare carnival!!!!
I want to pay differently for time, person, or AI
You can get a cheaper cut if you go to a barber school with a barber in training. If you go to an academic medical center and a resident is overseeing your care, you definitely do not get a discount lol. You get a very tired guy named Dr. Neil that asks you questions while filling in your patient record and then you’re billed under the attending at full price.
Today people like to debate “who is liable if something goes wrong?”, when a more interesting and uncomfortable question is “how much risk should patients be allowed to take?”. The ethics question people don’t want to grapple with is whether your ability to pay should govern if you get better or worse care.
But maybe we should let people choose their risk and pay different amounts accordingly. This will also end up changing how long your wait times are since it will likely change the demand curves.
- You can talk to a chatbot that can handle 50 common issues (including prescribing and order labs) and you’ll pay $10 and get seen immediately. If the chatbot can’t handle it, then you get triaged up.
- An on-demand virtual medical team can see you within 2 hours and you’ll pay $25
- A nurse + AI wraparound can see you in 2 days and it’s $40
- A primary care physician at a name brand hospital can see you in 1 week and it’s $60
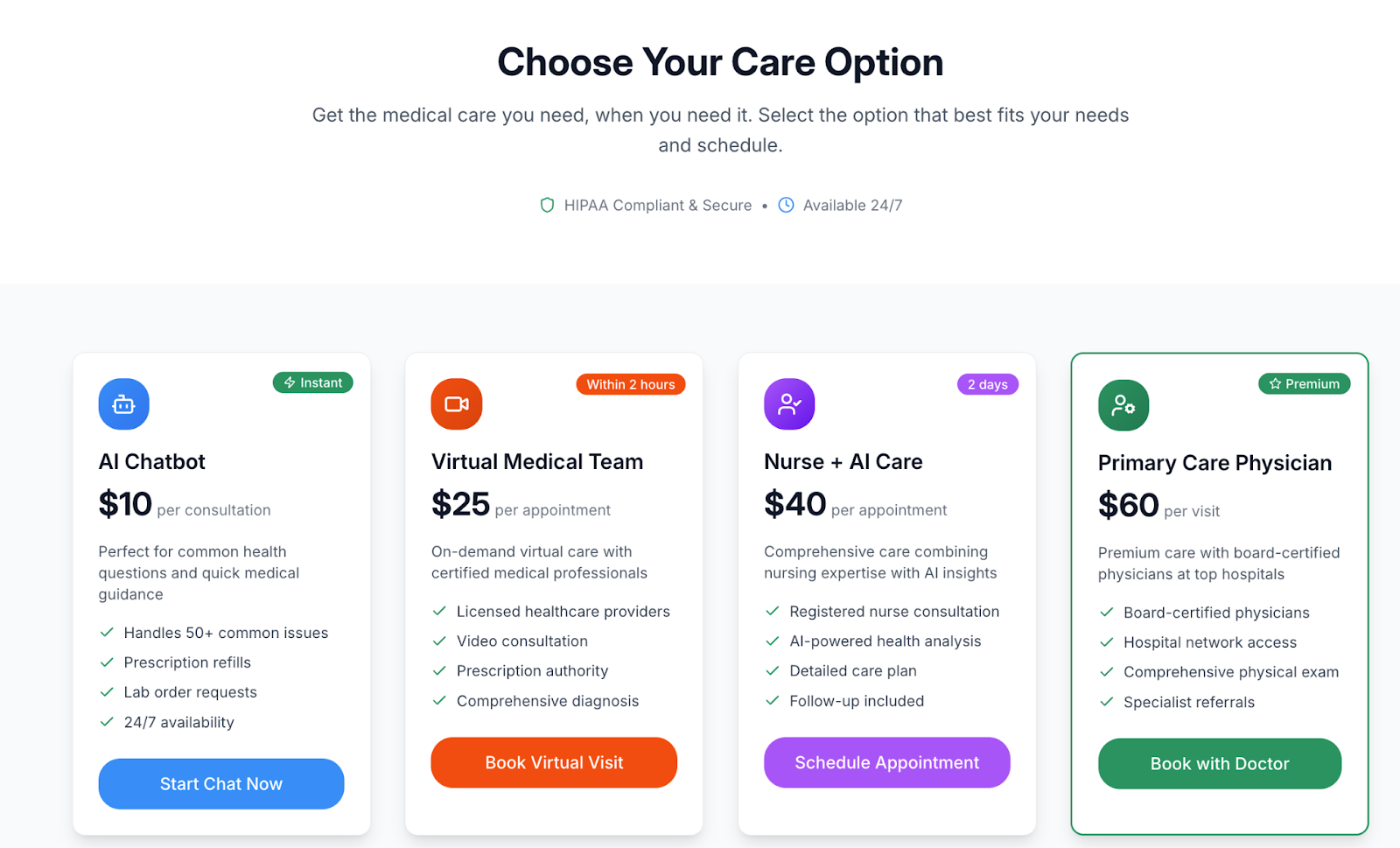
You could segment this in all sorts of ways - I picked them arbitrarily to show that risk and quality are subjective and random. But this is a way for patients to make that choice themselves. I probably don’t need to spell out all the things that could go wrong in this one…but maybe patients would prefer to be able to choose themselves!
Let me build my own medical equipment at home
Related to the “should patients be able to risk themselves” discussion…durable medical equipment (DME) is an area where patients are already experimenting at their own risk.
- OpenAPS helps patients hack together an automated pancreas through an open-source software package, continuous glucose monitor, software package, etc.
- Organizations open-source files to create 3D printing prosthetics
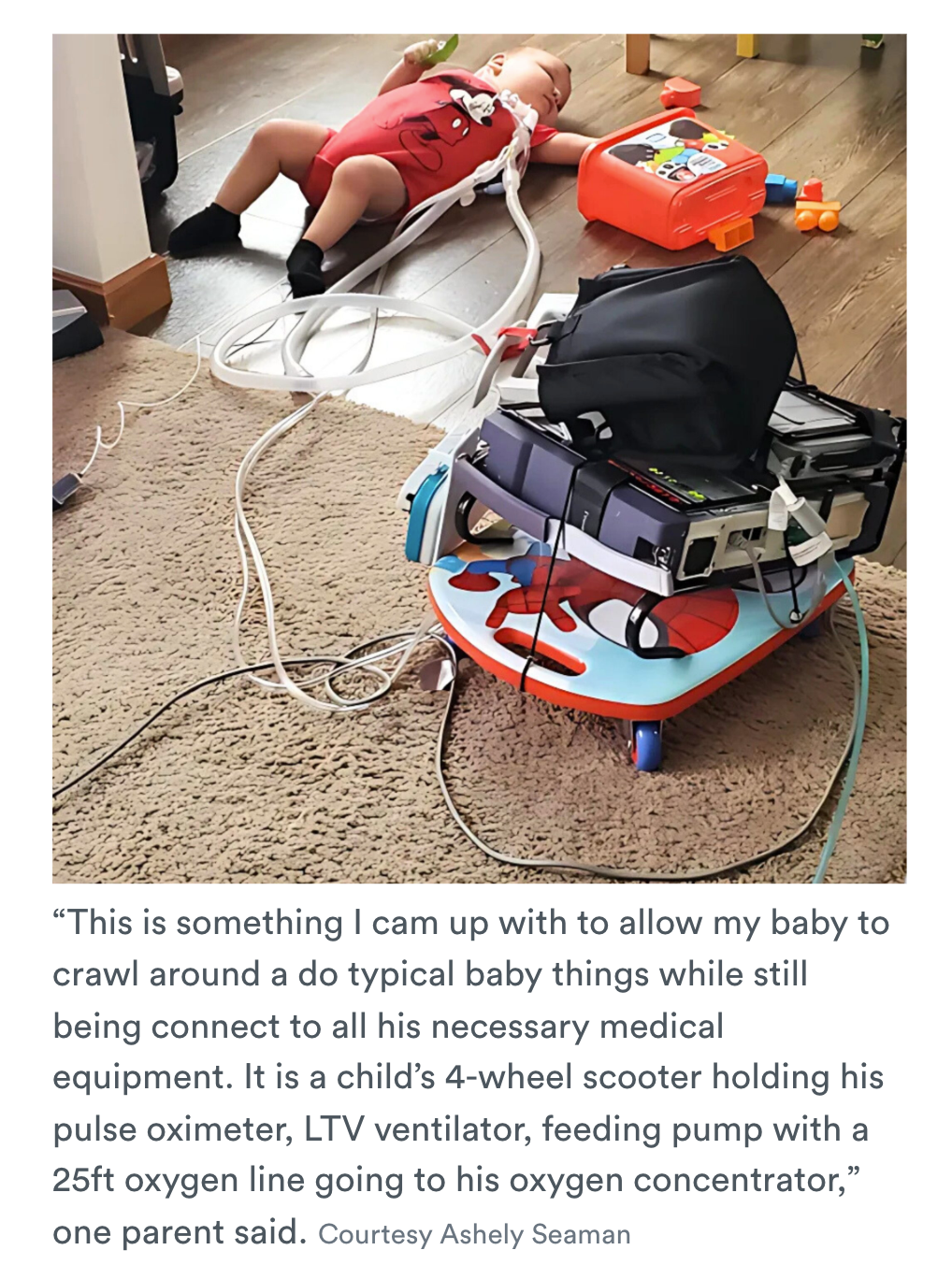
- Parents of children with complex medical needs are making their own DME adjustments that manufacturers won’t do themselves or payers aren’t willing to pay for.
The reason this is happening is probably a few fold. First, durable medical equipment companies generally don’t get paid more for small increases in quality of life they bring to patients, so patients have to do that themselves. The second is you might not be able to afford the DME cost since a big chunk is usually out-of-pocket.
But right now it’s pretty binary. Either it’s DME that is approved to be covered by an insurer and it’s incredibly expensive, or patients are navigating gray areas and online forums to figure things out themselves and take on the risk if things go horribly wrong. Maybe there should be a middle path of “well if you’re going to do this yourself…here are some open-source packages we’ve vetted and we’ll give you $100 to buy the materials. Good luck and the risk is on you!”
Prediction markets for patients
At the last hackathon jokingly had one idea about making prediction markets for patient outcomes. I thought it was funny, but I have severe brainrot.
A couple of weeks ago, I saw a thread on Twitter of someone posting all their mysterious symptoms (cognitive decline, fatigue, etc.). What do I see at the bottom but…someone created a prediction market to guess this person’s diagnosis! I’m gonna be rich betting on this guy’s thyroid function!!!
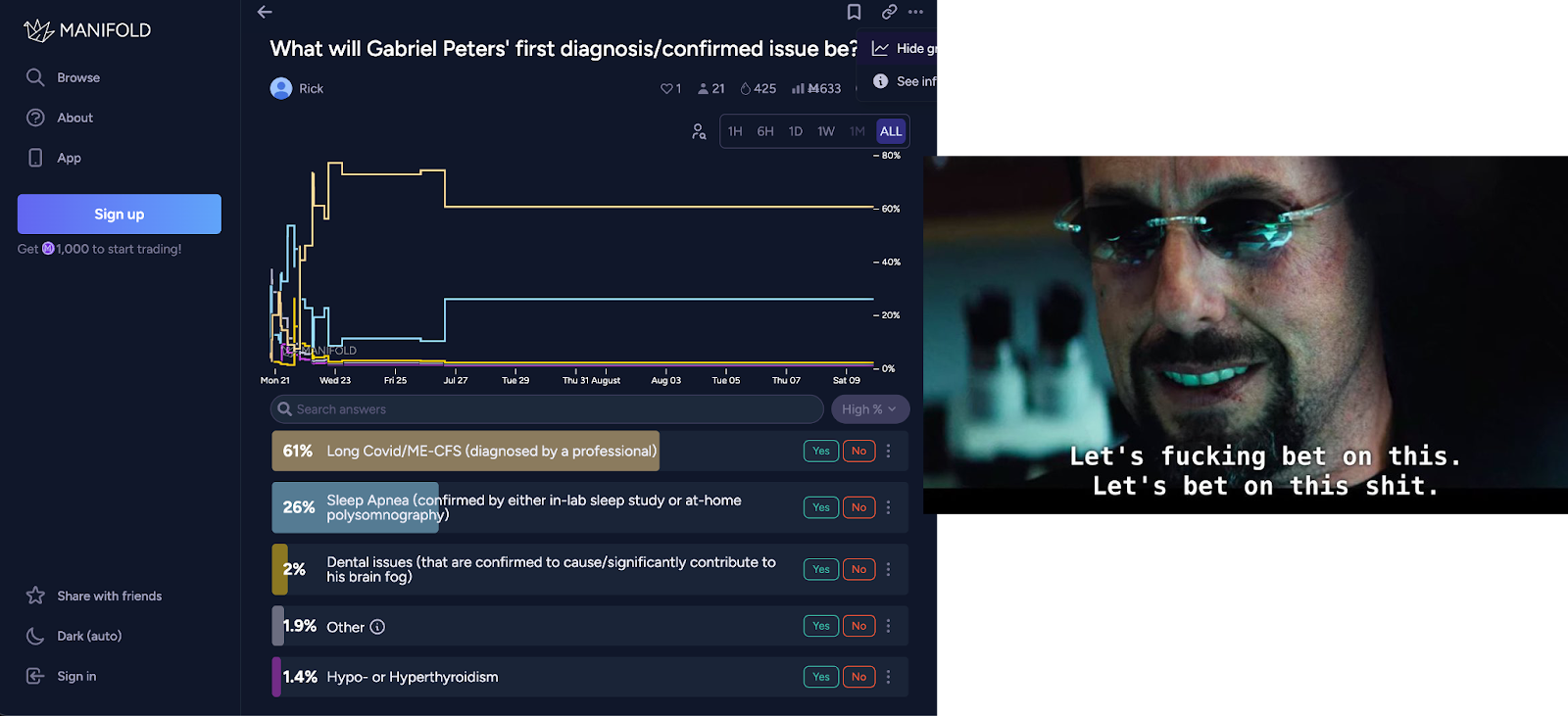
Maybe this is a more interesting way to get a second opinion. I put all of my symptoms out there, and then docs start betting on what they think I have in these prediction markets. I use that to figure out whether it’s worth getting a confirmatory diagnosis based on the results, and then payouts happen once I see another doc.
But that’s the boring version! I have a better idea - how about if you’re a diabetic, you can create a prediction market about whether your A1c levels are going to stay within range for 6 months. The haters can bet against you and it’s tracked via a continuous glucose monitor. If you go out of range too many times, it auto pays out the haters. But if it doesn’t, the haters pay you!
Once again, let’s ignore the ethics of this. Like…if I’m betting that you won’t do the healthy thing, I might actively sabotage your life. Or if I make a prediction market on whether I have long Covid, I might go to a “friendly” doc to diagnose me and split the winnings.
But what could be the positives of something like this?
- Patients get paid for doing healthy behaviors. This is something I’ve said doesn’t work in the past. But this is different because there’s a person that will actually pay you for this - haters that don’t want you to succeed but are proven wrong. On the flip side, there’s also downside risk for the patient for not succeeding so they have stronger incentives to succeed. It’s micro-level value-based care! Powered by haters!
- You might actually build a more interesting risk-triaging system - what do the crowds (or even people closer to the patient) think about their riskiness? When a patient posts a “should I wait or go to the ER” question on reddit, people could bet on it and give a real sense of risk to the patient.
- You could discover population level risks more quickly via patients reporting their data. If a patient on a drug is experiencing side effects, they might bet on a recall or safety label change. This might actually increase the number of patients that report side effects to the FDA, and give us better data about drugs directly from patients.
- Patients could upload their documentation and explanation of benefits and bet on whether their payer will cover it or what the final will be. This could get a dataset of contracted rates between payers/providers, or help providers change the care plan if they think it won’t get covered.
Remember kids, everything is a casino now. Why shouldn’t our healthcare???? I want to BECOME a meme stock, not just invest in them.
Conclusion and Parting Thoughts
Which of these ideas would you be down for? Which ones do you think are too ethically fraught?
I do think in general we’ve swung a little too far on the paternalism side when it comes to US healthcare. Patients aren’t allowed to make many choices themselves but have to keep paying the ever increasing prices. Even if it turned out to be catastrophically wrong, I think more patients would at least understand it’s because of a choice they made and feel agency in the situation.
Or idk maybe I have a gambling problem.
Thinkboi out,
Nikhil aka. "Selling my body for money for my body"
Twitter: @nikillinit
IG: @outofpockethealth
Other posts: outofpocket.health/posts
{{sub-form}}
If you’re enjoying the newsletter, do me a solid and shoot this over to a friend or healthcare slack channel and tell them to sign up. The line between unemployment and founder of a startup is traction and whether your parents believe you have a job.
Quick Interlude - NEW COURSE ON FHIR! KNOWLEDGEFEST APPS DUE SOON!
See All Courses →So...what actually is FHIR? I get this question a lot, but there's never really enough time to explain it and also I would just mumble "technical standard" and walk away.
So we decided to do a standalone free FHIR 101 course in partnership with Redox! Over 3 days in August we'll go over the spec itself, how it differs from other healthcare information standards, and practical tips to build with it.
I wanted to call it FHIR fest but it got nixed. You can sign up for it here, it's FREE and it's 8/25-8/27.

And a reminder that Knowledgefest apps are due this week. If you want to be in a room with the best ops people in healthcare, you should apply like TODAY.
We sell this conference out every year - all workshops, learn how people are building and scaling in healthcare, application based so we only take the best. We have people from Commure, Clarity Pediatrics, Pomelo, and Waymark already coming, join the squad.

Get Out-Of-Pocket in your email


