




Who's Supervising Your Nurse Practitioner?
Get Out-Of-Pocket in your email
Looking to hire the best talent in healthcare? Check out the OOP Talent Collective - where vetted candidates are looking for their next gig. Learn more here or check it out yourself.
 Hire from the Out-Of-Pocket talent collective
Hire from the Out-Of-Pocket talent collectiveHealthcare 101 Crash Course
%2520(1).gif)
Featured Jobs
Finance Associate - Spark Advisors
- Spark Advisors helps seniors enroll in Medicare and understand their benefits by monitoring coverage, figuring out the right benefits, and deal with insurance issues. They're hiring a finance associate.
- firsthand is building technology and services to dramatically change the lives of those with serious mental illness who have fallen through the gaps in the safety net. They are hiring a data engineer to build first of its kind infrastructure to empower their peer-led care team.
- J2 Health brings together best in class data and purpose built software to enable healthcare organizations to optimize provider network performance. They're hiring a data scientist.
Looking for a job in health tech? Check out the other awesome healthcare jobs on the job board + give your preferences to get alerted to new postings.
TL:DR
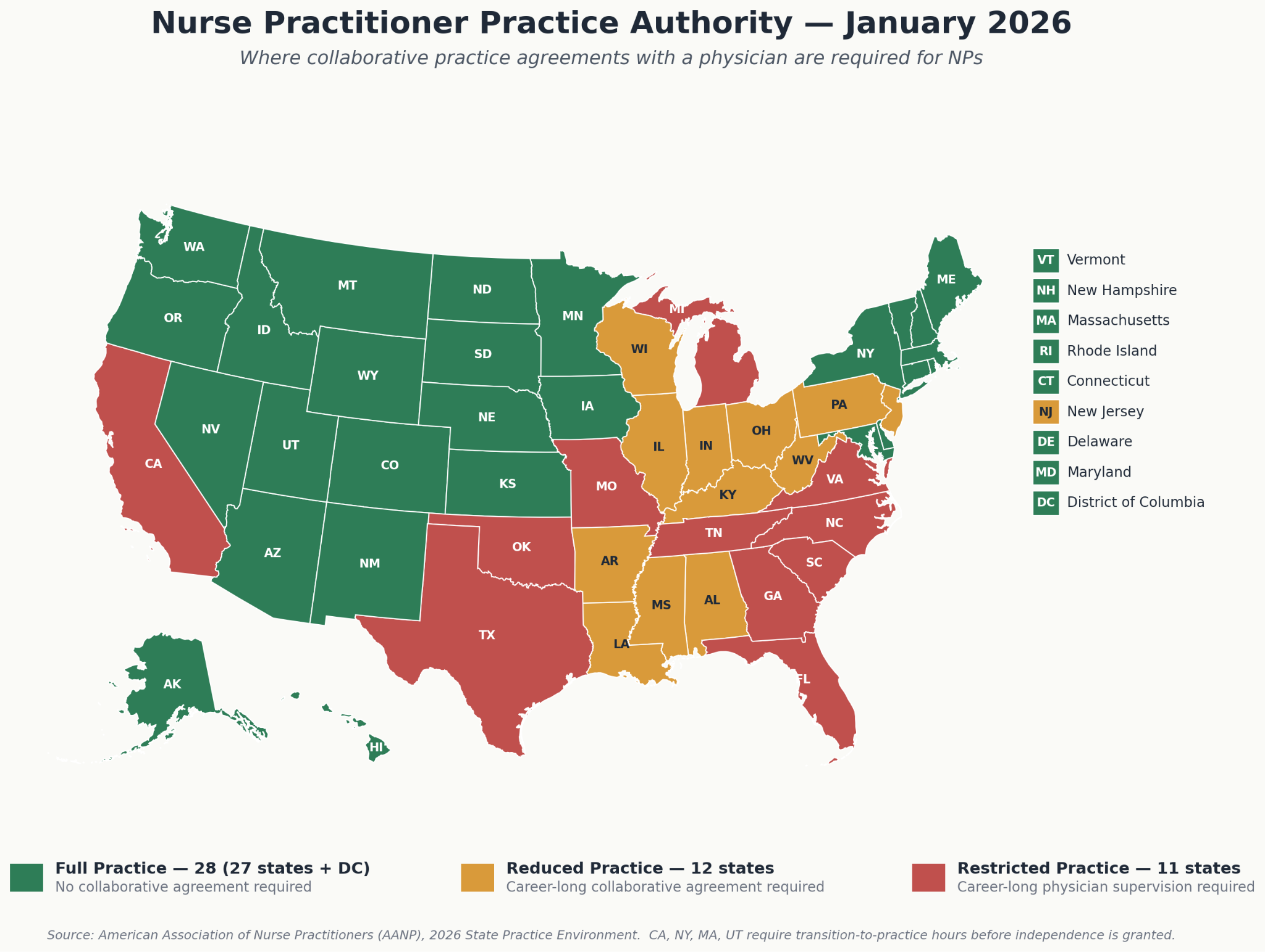
In roughly half of US states, nurse practitioners (NPs) and physician assistants (PAs) can't practice independently. They have to be in a collaborative practice agreement with a physician who reviews some percentage of their charts, signs off on protocols, and is supposed to pick up the phone when there's a clinical question. State enforcement has been picking up recently around whether these agreements are being done compliantly, especially in medspa and IV therapy.
GuardianMD matches NP/PA/and nurse-owned clinics with physicians. They are building a platform that helps with the oversight needed for chart review workflows, HIPAA-compliant messaging, on-demand telemedicine, escalation, and a state-by-state regulatory layer.
In the post we talk about the requirements for the collaborative practice agreements, the state-by-state variance, and the trends in favor and against GuardianMD.
—
This is a sponsored post. You can read more about my rules/thoughts on sponsored posts here. Wanna chat sponsorship? Hit us up.

Company Name - GuardianMD
The company is GuardianMD, and they provide the platform to enable collaborative practice agreements between non-physician practices and the physicians that oversee them.
The company url is Guardian “Medical Direction”. They have Medical Directors with Doctors of Medicine, some of whom practice in MarylanD. And those doctors are Managing Directors of the physician corps.
So can you guess what “MD” actually stands for???
What's The Pain Point Being Solved?
Most people would say we don’t have enough doctors in the US to serve the population, especially primary care doctors. In order to try and address that shortage, in the US we allow nurse practitioners and nurses to do certain functions docs can do (usually with some caveats).
I am not going to wade into the debate of whether this is good or bad. I have a family and a future I’d like to live to see. Anytime I see this debate happen online, it’s amazing to see two sides try to have a cancellation duel.
Instead I’d like to talk about the mechanics of how this happens. In states without full practice authority for NPs, they can't see patients without a physician on the back end. The physician's job, on paper, is to be available for consultation, review some percentage of the NP's charts, sign off on protocols, and in some states physically show up at the practice site. Physician assistants have a parallel set of rules that look different.
This is called a collaborative practice agreement, which outlines the responsibilities of the NP and the doc. Here’s a high level collaborative practice agreement that you can see yourself.
Every state has its own rules for what this relationship should look like and honestly has a lot of gray areas within it. For example:
- Supervision ratios - Texas allows a ratio of 7 NPs:1 Doc, Alabama allows 9:1. Ohio is 5:1 but Missouri and Michigan have no limit. New York is 4:1 if the NP has fewer than 3,600 practice hours (*points middle finger at Malcolm Gladwell*).
- Chart review cadence - How often is the doc supposed to review the NPs charts? Usually it’s 10% of charts the NP submits when the doctor requests. But how often that check needs to happen is usually not specified.
- Availability - The doc needs to be available for consultant, but what does “availability” even mean in 2026? Aren't we all on our phone 100% of the time and technically available even as our soul corrodes?
- On-site review - In some states the doc has to show up on site. Alabama requires the collaborating physician on-site for 10% of an NP's hours during the first two years. If they mess up, then it really is on sight.
- Specialty match - Do you need to match based on the same specialty? Florida requires a plastic surgeon or dermatologist for medspa oversight, or a felon if you wanna do durable medical equipment stuff.
That’s just some of the different state-by-state variance. For a single-location NP-owned clinic this is a headache. But for a multi-state IV therapy franchise or PE-backed medspa roll-up it's the whole game (besides helping hungover people).
The other issue is how do you find a doc that’s a good match for the right nurse practitioner? The doc needs to feel comfortable with the way the NP is practicing, and the NP needs to feel confident the doc is there to help them practice better. What does the doc’s availability look like and what’s the backup if they aren’t around?
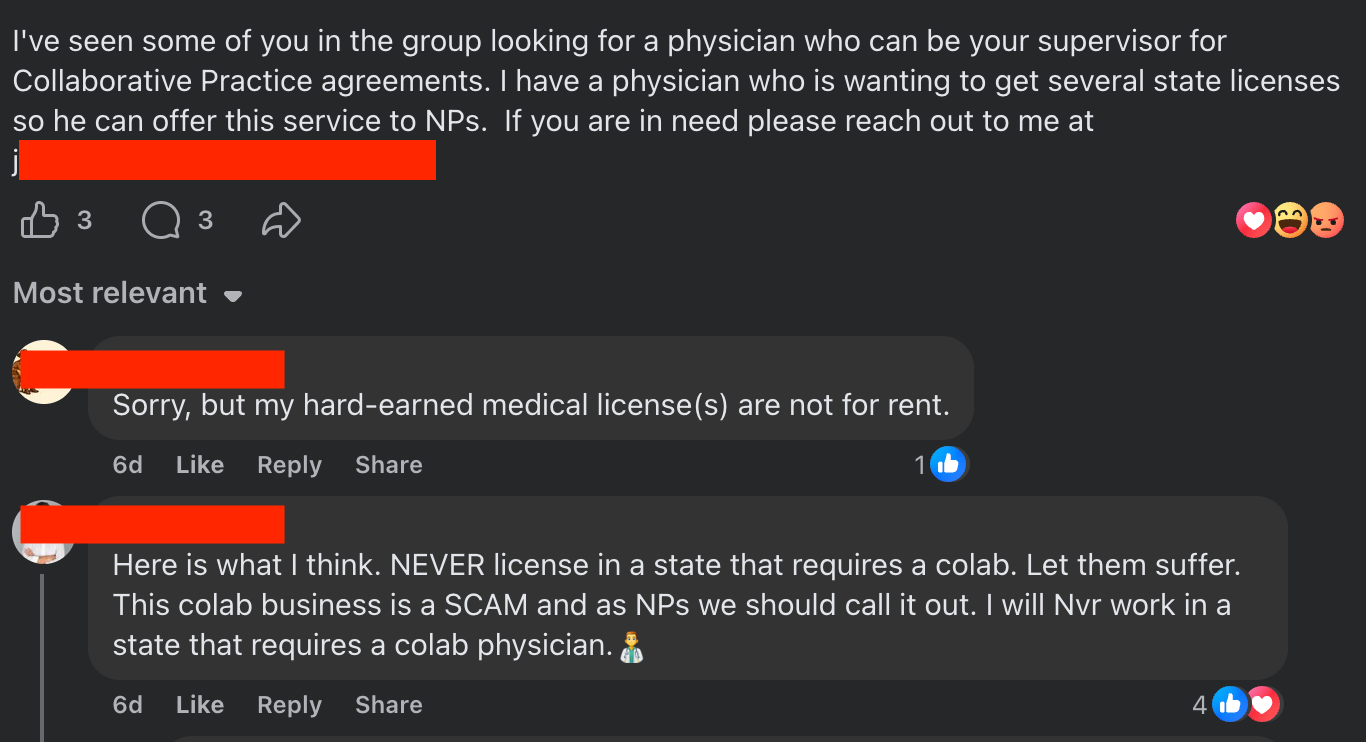
This has for the most part been a pretty gray market that’s been solved by Facebook/doctor groups online and word of mouth between NPs and MDs or headhunting firms that charge a one time transaction fee to make the match happen.
What Does GuardianMD Do?
GuardianMD wants to provide not only the matching between docs and NPs, but all the follow up services that would actually help the docs give oversight to the NPs.
When a new clinic joins they get a checklist of things they need:
- A clinic-MD agreement filed at the state level
- Their licenses uploaded
- What are the clinical protocols they have in place
- A list of phrases like “prior auth sucks!” that you can say to create middle ground with other clinicians
- What malpractice do they have
- And more
GuardianMD provides standardized protocol templates with references and contraindications, plus a state-by-state guide on how collaborative agreements actually have to be filed.
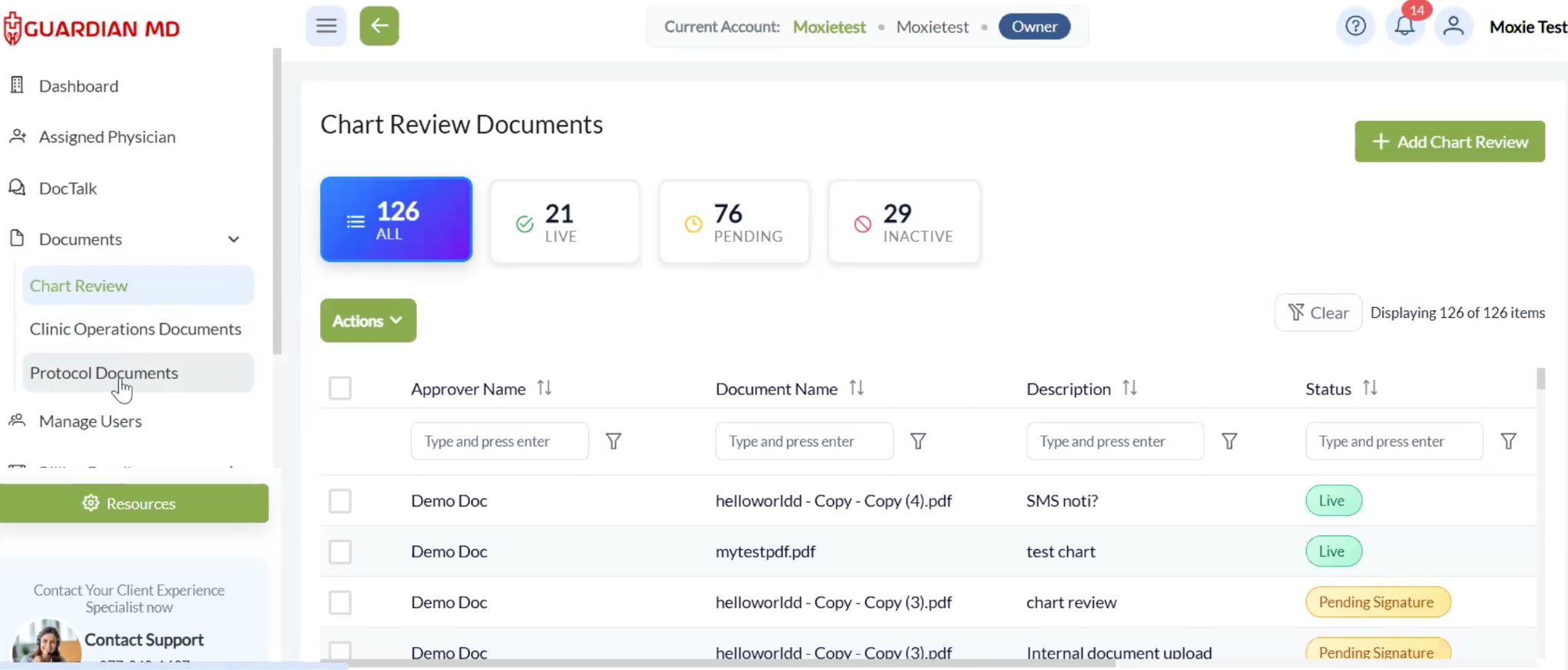
For chart review, NPs upload charts and the physician reviews them with a 48-hour signature SLA. The platform tracks which docs don’t do that, and if a doc is consistently missing a message then GuardianMD pulls them off the platform.
GuardianMD brings collaborating physicians, medical directors, telemedicine clearance exams, and chart review under a single network. It sounds simple but to set this up requires some complicated compliance mechanics that change per state.
This means one group is handling the collaborative agreement, the clearance exams, and the protocol sign-offs, rather than three vendors who've never spoken to each other. The chain of patient-provider responsibility stays intact instead of fragmented across separate vendors who've never spoken. If a clinic's primary collaborator is unavailable, another physician in the network covers without a gap.
For example they have a HIPAA-compliant messaging app inside the platform where NPs talk to their collaborating physician. GuardianMD has a centralized team of clinical staff that fill in the gaps if collaborating physicians don’t respond. A clinical ops team monitors the queue and can escalate. They’ll loop in a specialist (a cardiologist for an EKG read, a dermatologist if you need someone to talk about great work-life balance) or pull a doc into an on-demand telemedicine visit.
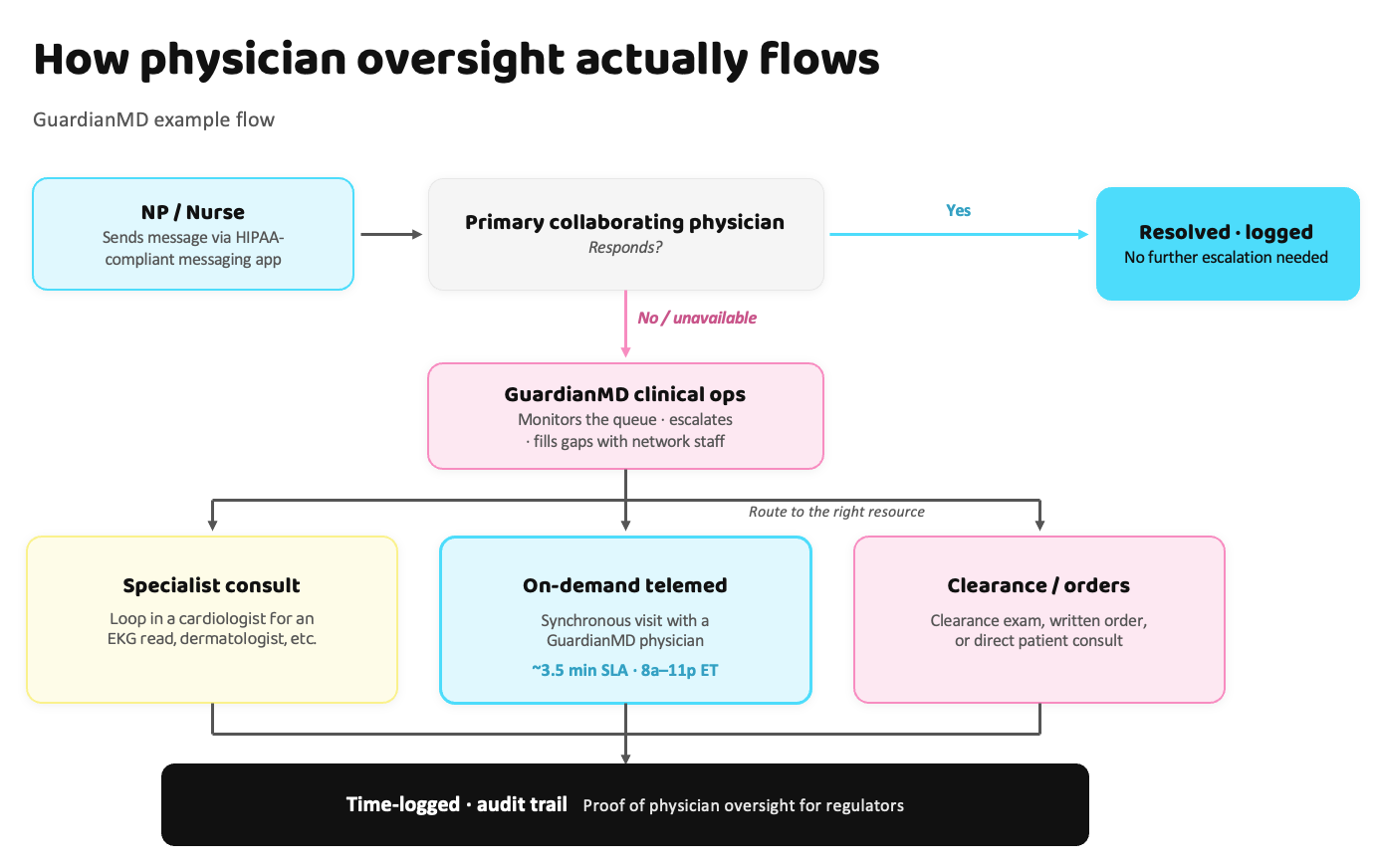
Or sometimes the NP or nurse needs a telemedicine visit for their collaborating physician to weigh in or do a clearance exam, write an order, or speak to a patient. They enable a synchronous telemedicine visit with a GuardianMD doc SLA is around 3.5 minutes from request to seen, 8 AM to 11 PM ET.
All of these are time-logged with an audit trail if regulators come and ask to see proof that there is actually physician oversight for these practices.
What Is The Business Model And Who Is The End User?
GuardianMD charges a subscription fee. The base medical director plan starts around $750/month; pricing scales with users (additional NPs, PAs, RNs) and complexity (multi-state operations, telemedicine volume, other compliance service).
They tend to focus on two areas in terms of clinics. One is wellness, aesthetics, IV therapy, and medspa brands. These are usually overseen by a nurse and have a limited number of clinical protocols. The other is primary care, behavioral health, urgent care and other specialty specific practices run by an NP which are higher complexity.
While they work with a lot of single clinic locations, they are increasingly working with PE groups and franchises that oversee multiple locations at once and want to eliminate the single point of failure risk for having one physician owner. Let the old head retire.

Job Openings
GuardianMD is looking for a few role, especially physicians that are interested in this kind of model. You can see more details here.
Out-Of-Pocket Take
A few things I think are interesting about GuardianMD.
Creating actual oversight into a gray area. Look, wherever you lie on the debate of “should NPs be allowed to practice like docs” the reality is that it’s already happening. While we’re in that current paradigm, we should have actual oversight into how these clinics are practicing and create real oversight/training for docs to assist.
In order to do that we need tools that formalize these relationships, track performance, and provide feedback. We need avenues where practitioners can ask for help and actually get it. And this can eventually allow clearer ways for good NPs to “graduate” and not need oversight.
This should make everyone a little happier. Or not idk y’all are grumpy.
Lowering the friction of starting a practice - Most NP- or nurse-led businesses stitch together separate vendors for their compliance stack. The chain of patient-provider responsibility fragments across companies that have never spoken, and arguments about who owns what surface the first time something goes wrong. Coordinating it through a single network + adding clinical protocol templates makes it way easier to launch.
Subscription payment alignment - By charging a subscription, theoretically GuardianMD needs to provide value on a recurring basis to their practices. This means they need to actually provide the support they say they’re going to vs. just matching the practices with physicians and then peacing out. So SMASH that SUBSCRIBE button for ARR.
A good foundation for other kinds of oversight - Another area for GuardianMD to expand could be pharmacist or unmatched med student collaborative practice agreements. States are exploring allowing both of these groups to offer certain kinds of services to patients under the supervising relationship with a doctor. Eventually we’ll see a Travis Scott collab at this rate.
---
Some things that could be challenging for GuardianMD:
Regulatory swings - One trend happening right now is that some states are giving full practice authority for NPs, which means they don’t need a collaborating physician to oversee them. A lot of NPs understandably are saying that the current collaborative practice agreements with absentee docs are basically a tax on them without actually helping.
But on the other hand some states are cracking down harder on corporate practice of medicine or restricting NP scope of practice in response to medspa misadventures. If we go down the route of full independence you might not need a GuardianMD, but if it stays in flux then it might actually help to have someone figure out each state for you.
Competition - The question is whether the value prop of everything above is worth paying for in the eyes of the clinic owner. You could get a doctor who'll sign a collaborative agreement for a few hundred bucks a month and not ask too many questions. It’s like a reverse sugar daddy.
As long as state enforcement is uneven, a meaningful share of clinics will rationally pick the cheaper, less-rigorous option. But if state enforcement does pick up, then you’ll need to retrospectively have a reasonable audit trail that shows there was physician oversight.
The scale constraints - A business like this is inherently constrained in scaling based on the doctor:NP ratios you need to maintain to provide reasonable oversight. It’s also constrained by the number of docs that want to participate, which are relatively fixed in supply and also deal with the same competition dynamics we talked about before + additional peer shaming dynamics.
There’s an open question of whether eventually you can increase the doc:NP ratio with AI as a reasonable middle layer to provide advice and auditing. GuardianMD could be in a good position for this shift by already tracking things like chart review and having audit trails for this.
Conclusion and parting thoughts
One day we can have the fight here about doctors vs. nurse practitioners. It will be an Avengers: Civil War style montage and we can see who takes sides.

But today, more care is being delivered by nurse practitioners and registered nurses. So instead of fighting, we should find ways to make it easier for the doctors to provide help and teaching to NPs/nurses so patients can get better care.
GuardianMD is making a bet that they can make collaborative practice agreements an actual collaboration instead of just a name.
Thinkboi out,
Nikhil aka. “Winguardian MDiosa” aka. “Physician x APP collab DROPPING this spring”
Twitter: @nikillinit
Other posts: outofpocket.health/posts
{{sub-form}}
If you're enjoying the newsletter, do me a solid and shoot this over to a friend or healthcare slack channel and tell them to sign up. The line between unemployment and founder of a startup is traction and whether your parents believe you have a job.
Interlude - Apply to Knowledgefest! And healthcare 101 starts next week!
See All Courses →Don’t forget the application for our Knowledgefest, our healthcare software engineering conference IS LIVE.
If you work in healthcare ops, you want to be here. This is where you learn playbooks, see what other ops people are doing, and build your network. It’s year 5 and we sell out every year - applications are due end of month.
And if you feel like you really need to get up to speed on how healthcare works, then you should let me teach you at Healthcare 101starting next week!This is for anyone hiring teams of non-healthcare people that need to get up to speed quickly (in 2 weeks) - we do group discounts too hit up ya boy. You’ll even learn how to make memes.
.png)
Get Out-Of-Pocket in your email


