




Using Marriage To Game Health Insurance (Theoretically)
Get Out-Of-Pocket in your email
Looking to hire the best talent in healthcare? Check out the OOP Talent Collective - where vetted candidates are looking for their next gig. Learn more here or check it out yourself.
 Hire from the Out-Of-Pocket talent collective
Hire from the Out-Of-Pocket talent collectiveHealthcare 101 Crash Course
%2520(1).gif)
Featured Jobs
Finance Associate - Spark Advisors
- Spark Advisors helps seniors enroll in Medicare and understand their benefits by monitoring coverage, figuring out the right benefits, and deal with insurance issues. They're hiring a finance associate.
- firsthand is building technology and services to dramatically change the lives of those with serious mental illness who have fallen through the gaps in the safety net. They are hiring a data engineer to build first of its kind infrastructure to empower their peer-led care team.
- J2 Health brings together best in class data and purpose built software to enable healthcare organizations to optimize provider network performance. They're hiring a data scientist.
Looking for a job in health tech? Check out the other awesome healthcare jobs on the job board + give your preferences to get alerted to new postings.
Marital status and fractured (but whole) risk pools
Listen…we all are looking at some crazy health insurance premium increases next year. So you should simply do what I did and get married. It’s not that hard lmao.
One thing that makes the US so wacky is that you can basically bop between insurance pools based on a number of different factors: income, military status, job, etc. When any of these changes, suddenly you have an opportunity to switch your coverage, and also which services are covered.
What this means is you can do some hacky stuff to optimize your health insurance coverage by tweaking these factors to get the right coverage you need. For example, we talked about enrolling in community college to access cheaper health insurance many years ago. Today we’re going to focus on another one…marital status.
My wife is a beautiful, smart, funny, and all around amazing person. These qualities are all secondary to the fact that she has good insurance.
Here’s an uncomfortable reality - out of all the benefits you get from legal marriage, getting access to your partner’s health insurance coverage is now one of the most important. Healthcare is one of the largest singular expenses that many households have now, so there's a good reason you’d use a marriage to optimize for this.
This is doubly true with a lot of people being out of a job and the individual exchange plans being particularly bad in 2026.

Today, we’ll talk about some ways you can do that. A disclaimer upfront: I don’t condone or endorse these things. In fact many of the things I’m about to explain actually make the risk pool actively worse and are extremely ethically dubious. In some states it’s potentially illegal.
I’m just pointing out that this is possible because we have a healthcare system that has this fractured risk pool. My hope is in the future we have a system that has some sort of single risk pool with everyone in it. Then it wouldn’t need these kinds of workarounds for people to get coverage.
Here are some ways you could TECHNICALLY alter your marital status in your favor depending on your health coverage needs.
Quick OOP announcements
2 quick course things
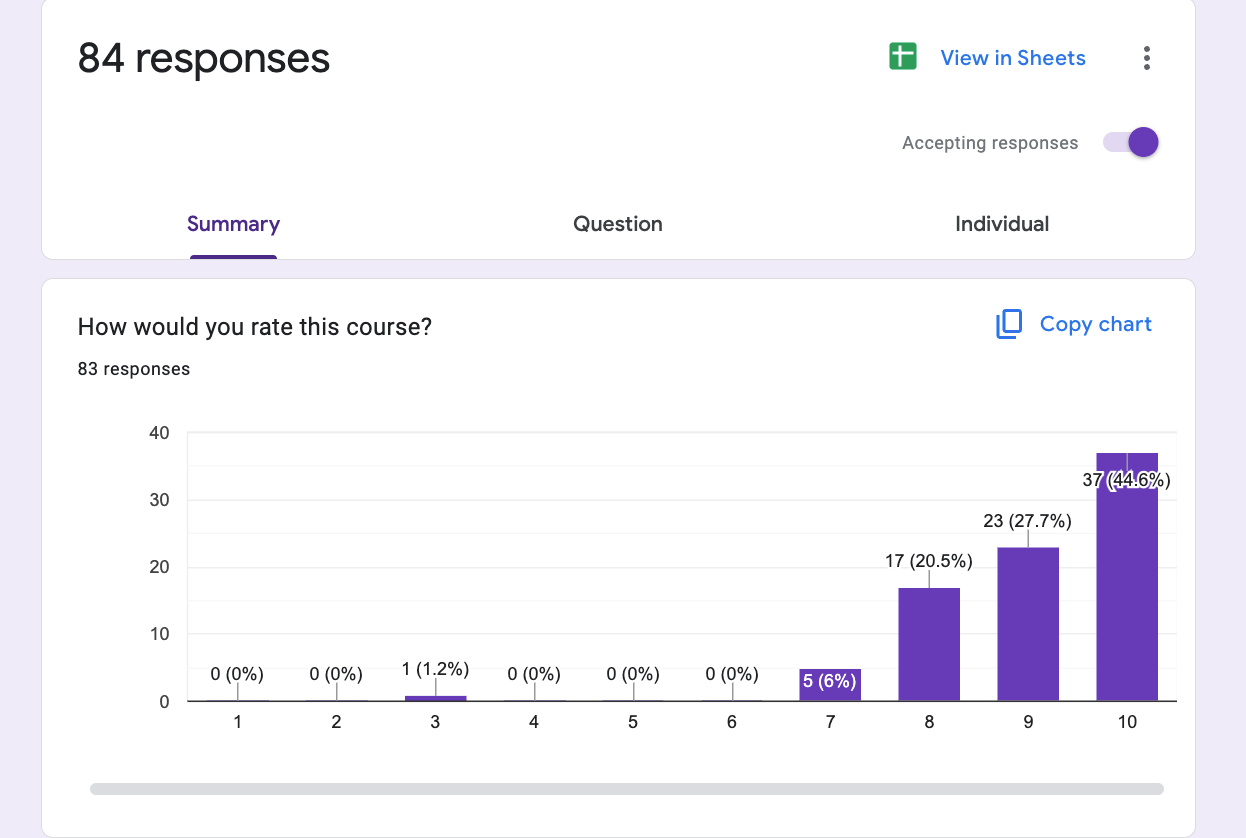
- Our FREE Value-Based Care course with Navina starts today. If you’re interested, this is your last chance to sign up! You’ll get the slides and recording even if you can’t make all the sessions live.
- Healthcare 101 starts 12/1!!! I’ll teach you everything you need to know about the basics of how US healthcare works. How the money moves, major laws, and trends happening in the space.
We do group discounts, plus everyone is leaving for Thanksgiving soon so bug your manager to get approvals now :).
Separately - we have a few seats that just opened up for our healthcare coworking spaces in Chicago and Boston. We’ll add more to SF and NY soon hopefully!
You can learn more and sign up here. We basically get remote employees/small teams in one space so we can learn from each other!

Back to tying and untying the knot.
{{interlude 3}}
Getting a Lightweight Marriage
If you’re dating someone and you have a relatively…lax view on what marriage means. Well, could you legally get hitched? I mean not to like, put a label on things.
At the lowest level, you could file for a domestic partnership, which is quite cheap ($30-50). While not legally mandated, many employers will consider this acceptable to enroll someone as a dependent. That’s when you change your Hinge filter criteria to people that work at those employers.

But many employers will only give health insurance with a legal marriage. Even if you’ve only been dating someone for a bit, you could technically get a legal marriage with a simple prenup for around $600. If you break up, an uncontested divorce will run you $500-$1500. Of course you need to double check.
So, you need to get around somewhere between $1100-$2100 worth of health benefits from the relationship to make this worthwhile. Considering how expensive coverage and healthcare goods/services are, that shouldn’t be too hard.
The big risks you take on here are:
- The person you get legally married to will contest the divorce.
- You’ll have to explain to a future partner that you have been legally married in the past and give an answer so lame you might actually get divorced again.
I don’t think anyone will actually do this unless it’s someone they’re informally married to - looking at you person who’s been dating someone for 8 years and “doesn’t believe in marriage as a concept”. But who knows, if premium increases get so high or you end up with a gnarly condition that needs better coverage, you might do crazy things.
Honestly I’ve seen people do more consequential things just to get laid. Getting technically married wouldn't be the worst.
Using Marriage to Create Special Enrollment Periods
Even if you plan to be with a partner forever, you can use the legal fluidity of marital status if you’re in a bind. Till death or premiums do us part.
Let’s say you’re pretty healthy, so you get the cheapest possible insurance or even go uninsured. But what happens if you fall unexpectedly very sick in the middle of the year? You could technically get married or divorced at that point to create a “special enrollment period” that then allows you to enroll in a new health insurance plan with better coverage. This coverage usually starts the next month you enroll, so it can’t be used for true emergencies, but can be used for really expensive care you know you’ll need (e.g. cancer).
Again, if everyone did this it would destroy whatever remnant of the risk pool is left. People would only sign up for coverage when they’re sick, and use marriage as a way to create a window to sign up. The social and literal costs of a divorce would normally prevent this, but the cost of coverage is now so high that it’s actually something people may weigh.
If you wouldn’t marry a homie to give them better health insurance, are you even a real friend?
Creating a Mom + Pop Shop for Small Group Plans
If both spouses are freelancers, you both have to get plans on the individual exchange. However, virtually all of the plans on the exchanges skew towards narrow network plans since most people are shopping on lowest premiums. Those plans might not have doctors you really want to see in-network.
What if you wanted to access a wider network plan in that case? In a few states (Texas, Louisiana, and South Carolina), you can create a two person company with your spouse to access the small group rates. There are some specific nuances per state on how this qualifies (e.g. putting them on payroll, ownership of the company, etc.).

But it does happen!
“Take Texas: Since 2016, none of the health plans on the ACA’s individual marketplace in Texas offer preferred provider organization, or PPO, plans.
Some insurers have allowed, for example, a husband and wife to create a limited liability company. They then count as an employer and employees, and can enroll in a small-group PPO plan.” - Stat News
Most other states have outlawed doing this or set more requirements on what counts as a small business (e.g. need at least one W-2 employee). But if you live in a state that allows this option, you could technically use it.
Spousal Incentive Health Reimbursement Arrangements
Everyone’s so focused on ICHRAs, they haven’t even looked into the abyss of other health reimbursement arrangements.
One of them is called a Spousal Incentive Health Reimbursement Arrangement (SIHRA). In this scenario, an employer would rather not cover the medical bills for you and your partner. So instead, they say “hey, if you get on your spouse’s plan instead of bringing them onto our plan, we’ll fund a wallet for you that will cover all your co-pays, deductibles, and other out-of-pocket costs”.
How it would work:
- You waive your company’s health plan and enroll on your spouse’s employer plan with a $2,000 deductible.
- Your employer gives you SIHRA with $2,000 in it.
- You get a $1,200 MRI. Your spouse plan processes the claim and gives you an explanation of benefits plus a bill.
- You’d upload that bill or explanation of benefits to whichever portal is used to process your SIHRA, and get reimbursed $1,200. You’d have $800 left to spend on co-pays, the rest of your deductible, and any other out-of-pocket expenses (but NOT premiums).

There are specific compliance things you have to watch out for here (how they interact with HSAs, how you prove you enrolled in another plan, etc.). But benefits consultants are talking about how employers saved $3.7M doing this!
Of course, this doesn’t actually save the system money because those dollars simply come out of a different employer’s pool. But you can shoot your shot and ask your employer if they’ll set one up for you!
Medicaid Divorce
Should we get dark???? Let’s say there’s something that is very expensive but Medicaid covers it. A common example is long-term care, which is frequently paid for out-of-pocket but costs a lot of money. If you can’t afford it, you can end up draining down all of your assets as a couple.
So what if the person that needs long-term care transfers all of their assets to their spouse, and then gets divorced? They’d then be low-income enough to qualify for Medicaid while the spouse then protects their assets. This is a very American sentence.

This was a strategy that was used back in the day. However, today it’s not REALLY done anymore because in most states, Medicaid will look back at your past 5 years of assets to see if you qualify (so you can’t make these big asset transfers). Also, “spousal impoverishment protections” were passed that offer similar-ish protections so that long-term care doesn’t totally bankrupt you (good summary of this here if you’re interested).
There are specific scenarios where it can still make sense to consider, like if you have a large amount of shared assets and one person might be requiring intensive long term care for a very long period of time. Even then, it still depends on what state you’re in and whether you want to take on the legal risk of a court saying it’s considered an uneven split.
But there are law firms that seem to specialize in this, which suggests it’s still something people consider. Or that law firms never update their sites, also plausible.
Featured Jobs Of The Week
Some companies are hiring, check them out!!!
Big Leap Health - Head of Revenue Cycle Management (New York City, NY)
- Come build foundational RCM infrastructure and teams at Big Leap! We're the AI-enabled business in a box platform for outpatient clinics offering breakthrough mental health treatments. We work with hundreds of clinicians today; we're looking for a tech-savvy RCM leader to take us to the next level. Apply here.
Autonomy Health - Founding Engineer (New York City, NY)
- We're on a mission to bring back private practice. Autonomy Health is an MSO empowering neurologists to launch, own, and operate their own practices, because physicians with more autonomy provide better care. Join us in transforming neurological care from the ground up. Apply here.
Conduit Health - Strategy & Operations (New York City, NY)
- Conduit Health helps chronic-care patients get what insurance should cover. We’re hiring a Special Projects wizard to build from zero to one, working directly with the CEO to stand up new teams and initiatives. Perfect for a future founder. Apply here.
Conclusion and Parting Thoughts
Dating is broken. But we can solve it by simply making health coverage worse and forcing people to marry into better coverage. Introducing my new dating app….

Again, I don’t think any of these ideas are broadly good for society. The ability to switch between different risk pools so easily is one of the core problems of US healthcare. Most of these are unethical loopholes that you can technically use, but if the situation becomes bad enough, there’s no doubt in my mind people will use them.
And if you get in trouble for doing any of the above, remember, none of this is real advice. Except try to get legit married, that shit is great.
Thinkboi out,
Nikhil aka. “my attachment style is insurance-dependent”
Twitter: @nikillinit
IG: @outofpockethealth
Other posts: outofpocket.health/posts
{{sub-form}}
If you’re enjoying the newsletter, do me a solid and shoot this over to a friend or healthcare slack channel and tell them to sign up. The line between unemployment and founder of a startup is traction and whether your parents believe you have a job.
Interlude - Apply to Knowledgefest! And healthcare 101 starts next week!
See All Courses →Don’t forget the application for our Knowledgefest, our healthcare software engineering conference IS LIVE.
If you work in healthcare ops, you want to be here. This is where you learn playbooks, see what other ops people are doing, and build your network. It’s year 5 and we sell out every year - applications are due end of month.
And if you feel like you really need to get up to speed on how healthcare works, then you should let me teach you at Healthcare 101starting next week!This is for anyone hiring teams of non-healthcare people that need to get up to speed quickly (in 2 weeks) - we do group discounts too hit up ya boy. You’ll even learn how to make memes.
.png)
Get Out-Of-Pocket in your email


