




Severe Mental Illness and the firsthand approach
Get Out-Of-Pocket in your email
Looking to hire the best talent in healthcare? Check out the OOP Talent Collective - where vetted candidates are looking for their next gig. Learn more here or check it out yourself.
 Hire from the Out-Of-Pocket talent collective
Hire from the Out-Of-Pocket talent collectiveHealthcare 101 Crash Course
%2520(1).gif)
Featured Jobs
Finance Associate - Spark Advisors
- Spark Advisors helps seniors enroll in Medicare and understand their benefits by monitoring coverage, figuring out the right benefits, and deal with insurance issues. They're hiring a finance associate.
- firsthand is building technology and services to dramatically change the lives of those with serious mental illness who have fallen through the gaps in the safety net. They are hiring a data engineer to build first of its kind infrastructure to empower their peer-led care team.
- J2 Health brings together best in class data and purpose built software to enable healthcare organizations to optimize provider network performance. They're hiring a data scientist.
Looking for a job in health tech? Check out the other awesome healthcare jobs on the job board + give your preferences to get alerted to new postings.
TL:DR
firsthand uses a combination of peers, care navigators, and technology to engage Medicaid enrollees with severe mental illness and help them begin their care journeys. They work closely with Managed Medicaid plans who pay firsthand to engage their members and share the savings firsthand generates. As the company scales, it will have to figure out how its model can scale while maintaining engagement and whether their model is a good fit for taking on increasingly more financial risk.
Also I got to do a ride around with the team in Memphis, so there are some pics of me being cute.
This is a sponsored post - you can read more about my rules/thoughts on sponsored posts here. If you’re interested in having a sponsored post done, email nikhil@outofpocket.health.
Company Name - firsthand
firsthand helps treat patients with severe mental illness utilizing teams of peers, care navigators, and technology. Yes their company name is all in lower case, idk if they’re like a super gen Z influenced company or just wanted to stick a massive middle finger to Microsoft Word autocorrect.
Their name comes from the fact that they want everyone to see severe mental illness (SMI) firsthand. I pointed out this was a pun to absolutely uproaring raucous laughter, I was the first person ever to point that out.
But their CEO Samir told me I need to go to Memphis to see how this model works…firsthand. We absolutely guffawed again. I was given a plaque for funniest person of the year.
After 20 times making the pun I explained that it wasn’t going to be possible, I was rolling out the course and there weren’t really any days I could make work. Samir then told me there would be…problems if I wrote about this…secondhand.
So anyway here I am in Memphis.

What pain point does it solve?
There are a few key pieces of context to understand before getting into how this company works.
First, most states today use private health insurance carriers to handle the state’s Medicaid program. This is called Managed Medicaid, and the carriers are called Managed Care Organizations (MCOs) in these arrangements. Why are they called something different here? Because this industry fucking hates you.
A state will put out a request for proposals (RFP) saying the kinds of things they want a Managed Care Organization to be good at when taking care of their Medicaid population, and then the MCOs submit bids. If they win, they’re usually given some lump sum $ per person in the plan and then have to take care of the Medicaid beneficiaries underneath that amount +/- bonuses and penalties for hitting certain quality metrics.

A few things are happening in this process that will become relevant later.
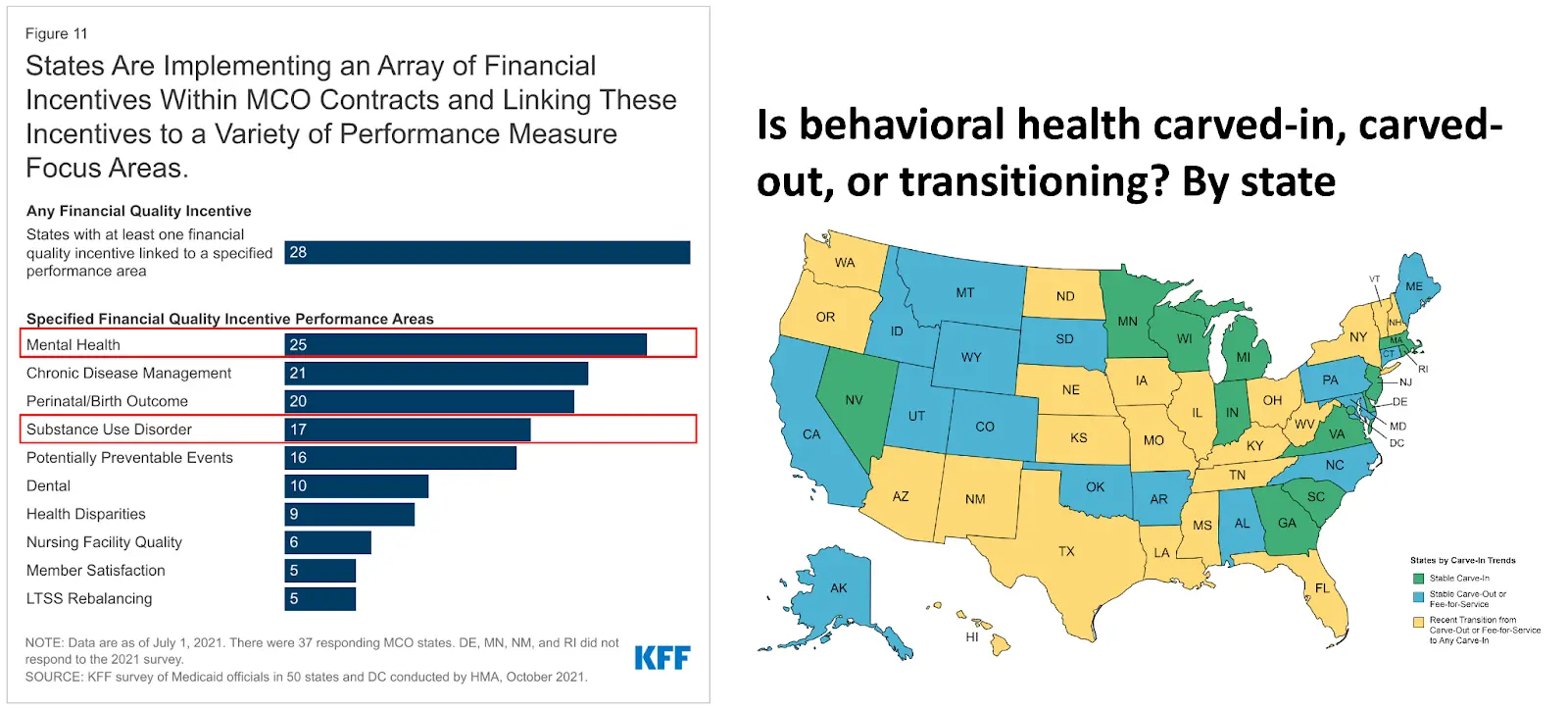
- Behavioral/mental health services were traditionally not included in this contract, it was only for “medical”. But in the last decade, more states are now “carving in” mental/behavioral health spend so that the health insurance carriers get more money to coordinate both.
- As fewer providers are available who take Medicaid (especially in mental and behavioral health), many patients find themselves in the emergency department as one of the few places they’re able to get care. These carriers try very hard to prevent unnecessary emergency department visits since it’s so expensive.
- More and more of these state contracts are including bonuses or penalties related to mental health and substance use in their request for proposals since it’s become an increasingly large problem within states.
- These health insurance carriers will get lists of people that they now have to cover with whatever contact information is on record. They then need to find these people they’re attributed to.
- These RFPs are getting longer and more boring. There’s no way someone is actually reading this. Are those people okay?
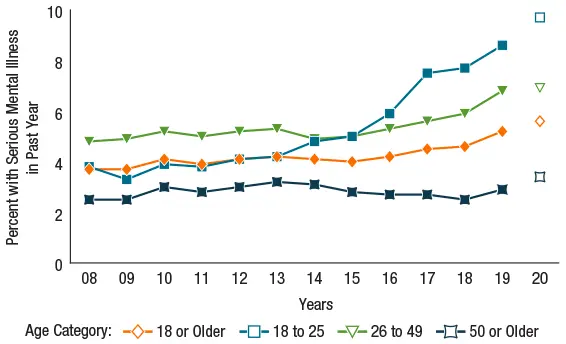
So all this Managed Medicaid stuff is happening on the government side. Meanwhile, the rates of severe mental illness (SMI) are increasing. Severe mental illness is defined as mental/behavioral health issues that cause functional impairment by limiting one or more major life activities. Think schizophrenia, substance use disorder, bipolar disorder, etc. There were 14.1M adults with SMI in 2021 compared to 8.3M in 2008.
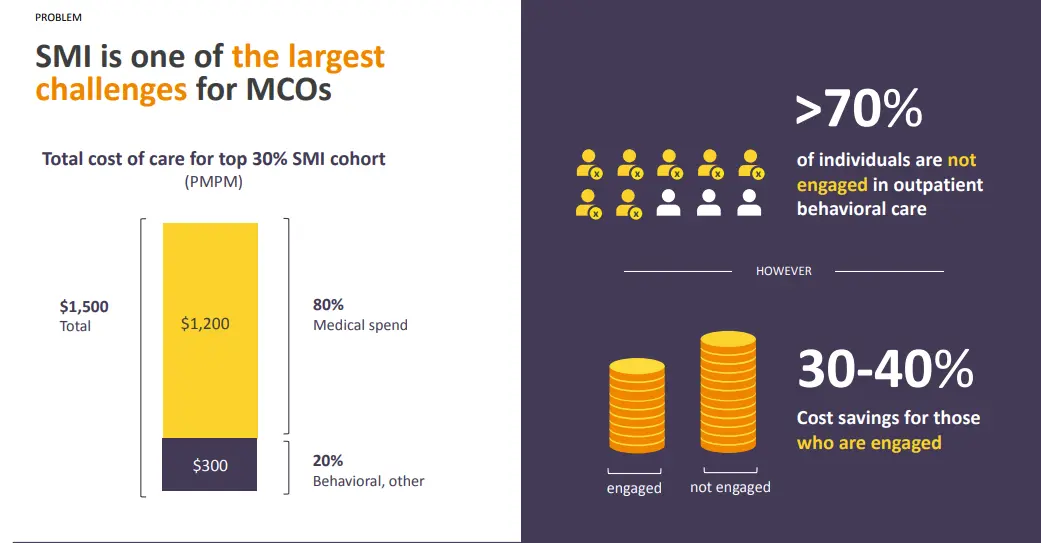
These patients are very expensive. firsthand showed me some of the internal payer data cuts around spend for patients with SMI. The most expensive patients are costing Managed Medicaid plans $1,500 per month! But also, interestingly, if you compare two similar patients with SMI, the ones who see someone regularly are 30-40% less expensive. For patients with SMI, the right combination of medications, dosing, and clinical interventions can dramatically improve their quality of life and manage their condition. But they require patients to be getting care, and less than half go to an outpatient facility in a given year.
When you put all of these together, there seems to be room for new SMI players who can engage these patients and save Managed Medicaid plans money.
What does the company do?
firsthand engages patients experiencing severe mental illness using a combination of technology, peer support, social workers, and care teams.
The main use of technology happens in the background to support frontline teams. The company does a lot of interesting data science work to help find patients. They’re given a roster of patients that they need to engage and usually the list is 80% incorrect in terms of contact information, address, etc. They mine claims data, health information exchanges, LexisNexis, etc to find general areas patients might be based on where they utilize care. They also score those patients based on how likely they think they’ll be able to engage them + whether they think they can meaningfully reduce costs for that patient. firsthand then sends these rosters to the field teams who can go out to engage these patients.
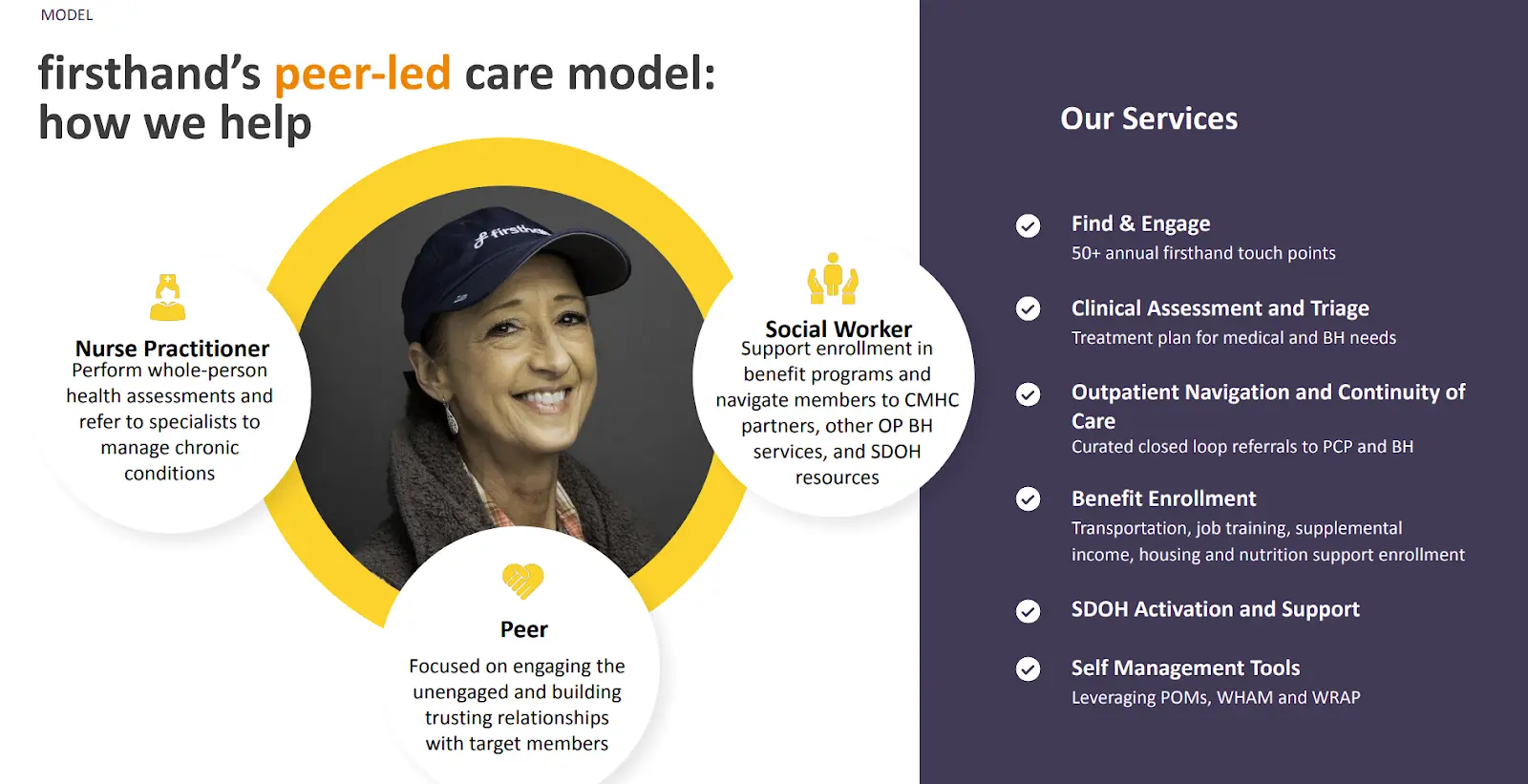
The real special sauce though is the peers. firsthand employs peers who themselves have some form of SMI that they live with on a day to day basis. These peers are trained on how to help others achieve health goals via programs that credential them as Certified Recovery Peer Specialists (CPRS). These peers go out to engage these patients experiencing SMI and use their lived experience to build trust and help them to start and continue their treatment. The peers drive them to appointments, check in on them, and act as a point of contact.
firsthand also provides the field with software tools that help them prioritize certain actions, like which members they should try to engage first. Or it recommends suggestions to field teams as they engage individuals like giving prompts that individuals have an upcoming appointment or medication may be running out.
In addition to the peers, each market has social workers to help patients enroll in services (transit vouchers, disability, housing, food benefits, etc.) as well as a nurse practitioner who helps oversee the patient’s health and coordinates their care with local clinicians (primary care, community mental health centers, etc.).
Some notes from being on the ground and seeing it in action:
- Local knowledge really matters here. For example, peers might ask around in areas where they think a patient might be and locals will know where to find them. Or a patient came into the office while I was there and they needed a fridge to store food, and the director knew a store down the street was going out of business and selling cheap fridges. It’s one thing to read about how “community knowledge” is useful in some consulting whitepaper, it’s another to see it yourself.
- Peers having their own history with SMI clearly resonates with patients. One member struggling with substance use came to the office while I was there, and having several of the peers in the office talk about their struggle with it + how long they’d been clean seemed to resonate. The patient and their peer left the office with a plan.
- The teams (peers, social workers, NPs) are tight-knit units within a given pod. Since the needs of SMI patients are so heterogeneous and expand through both clinical and social needs, a team-based approach is needed so the care isn’t fragmented. Teams do rundowns of all the issues and patients and they actually know many of each others’ patients by name. They also provide support and coverage for peers when needed, since many of them are also dealing with their own SMI issues that can come up.
- For many patients there’s an inherent distrust in the “medical system” as a whole. Peers don’t present as part of the medical system, and an effective tactic was using benefits like food to start the relationship with firsthand. Over time, peers can use that trust to loop in the nurse practitioner when the patient is ready to start the clinical journey.
- The barbecue absolutely slaps. Memphis knows what the fuck is up. The team asked me if New York had good barbecue and I was too ashamed to show them what we consider barbecue.

What is the business model and who is the end user?
firsthand gets paid by Managed Medicaid plans (e.g. UnitedHealth’s Medicaid plan in Tennessee). They only get paid if they manage to engage a member + they get a % of the medical savings that they’re able to reduce. In this way, they’re both incentivized to find and engage members + get them on the right clinical track to address their illness.
In more mature markets, they’re now shifting to taking on the full cost of patients even if they haven’t yet engaged them. This puts more financial risk on the company, but also gives them more $$ if they do a good job managing those patients. As they say, scared money don’t make no money.
The end users are patients who benefit from getting access to a point of contact for their health and social needs. The benefit is having a better handle on their severe mental illness and a path to recovery.
The health plans benefit from this relationship in a few different ways:
- They lower unnecessary medical spending by preventing unnecessary emergency department and inpatient visits.
- They’re able to help these health plans hit certain quality measures like follow up after psychiatric hospitalizations (FUH), diabetes screening for people with schizophrenia or bipolar disorder (SSD), etc. which give them bonus payments from the state or avoid penalties for missing them.
- They look good to state Medicaid directors since mental illness is a high priority for states especially when it comes up for contract renewal with the health plan.
- They atone for the sins of every other awful patient engagement strategy they’ve attempted. If I get one more piece of mail from them I’ll need to learn origami out of necessity.

Job Openings
firsthand is hiring for a bunch of roles, including:
And many more, including roles with field teams in Ohio and Tennessee. You can see the full list of roles here.
___
Out-Of-Pocket Take
I’m glad more companies are trying to build in the SMI category. I think the patients are criminally underserved, incredibly complex, and can really be helped with the right interventions. There are lots of things to like about firsthand.
The use of peers - I’ve talked extensively about this in the past when it comes to areas I’m investing, so I don’t want to seem like some bandwagoner here. But I think the peer model is especially important in something like SMI where half the battle is convincing patients that they need to start on the path to treatment. Seeing someone with your condition that is further along the treatment journey can be an excellent motivating tool + patients know they’re talking to someone that can empathize and is without judgment of their situation.
I asked Samir about whether firsthand has ever had a patient become a peer, and he said that’s the goal. “If that happens then it’s clear we have had a profound impact on someone's life, have a flywheel, and that’ll be a milestone to celebrate”. I was kind of sad that this newsletter wasn’t a milestone to celebrate, but I hid the pain.
Peers are also great because they can supplement the specialists and primary care physicians in a given geography that are largely inundated and don’t have time to chase down patients to make sure they’re taking their meds, going to follow-up appointments, etc. The peers + care team can act as a conduit of relevant information to the PCPs/specialist. I think in some of these areas with clinician shortages, this model of doctor + peers can actually be better for both patients and the clinicians.
A specific patient type - One of the reasons the firsthand model works well is because they’ve found a very specific population that’s particularly good to attempt to take financial risk. These patients are:
- Typically completely unengaged with the health system
- Very expensive when they do show up
- Somewhat predictably not expensive if they do engage in regular care
Many other patient demographics have one or two of these characteristics (e.g. diabetes), but the sweet spot is all three because it means you can clearly show attribution that what you did measurably decreased cost. Of course you have to build a good strategy to actually engage patients and keep them compliant with their treatment, which is the hard part.
Technology as a support vs. key pillar - I think a lot of digital health services companies have focused on how tech is used to interact with the patient in scalable ways or claim the tech is their secret sauce. Apparently if you interact with a patient using jotform you can 10x your valuation 🤔. For firsthand most of the technology is stitching together off the shelf software and the secret sauce + focus are the field teams. The technology is in service of making their lives easier - the patients don’t even see it at all. For complex patient populations this feels like the way.
Many companies think that the use of technology is the differentiating factor and investors really want to hear that. But firsthand doesn’t need a lot of fancy technology to make the model work - it’s much more about contracting, utilizing care teams smartly, and building trust.
—
I think what firsthand is doing is important, but like any company there are going to be challenges ahead.
Scaling - A core part of this model are peers + care teams being able to give personalized attention to patients. That works right now because the patient panels are relatively small. But as the company scales, it means protocols are put into place, the number of patients each team has to see grows, and a culture where people with SMI can juggle a heavy caseload while effectively managing their own mental health inevitably will become strained. The metrics look pretty good today, but do they look the same as firsthand expands into new markets? As they start taking on financial risk? After this post propels them into stardom?

Those same questions apply to the firsthand’s economics. Tech-enabled services are tough to scale, and in Medicaid that’s doubly true since each state is radically different. How does the company avoid the diseconomies of scale that tend to happen with the operations of tech-enabled services business? And can they get Managed Medicaid plans in more markets to contract with them with these kinds of terms (on the hook for engaging patients first, then full risk second)?
Regulatory - Since the business is entirely focused on a government payer (Medicaid), it’s probably not surprising that regulation can be both a benefit and existential risk. One existential risk is each state changing their Medicaid benefits in a way that makes it impossible for firsthand to operate - adding working requirements, carving out mental/behavioral health, not expanding Medicaid, changing how attribution works, etc.
Another is the current trend of pushing more risks onto primary care providers and hospitals to take on the total cost of care of a patient. This means firsthand would have to subcontract with other providers - where they might have a weaker value proposition if the provider already engages and manages the care of a patient. Or they might not be able to get enough money as a subcontract from these providers since they’re smaller and have less money to work with themselves.
Competition - There are several competitors entering the SMI space, each with a different plan to engage patients, different milestones they need to hit to get paid, and different staffing considerations depending on the level of clinical complexity they want to be able to handle. The firsthand model seems to work well in their current arrangement where they get paid for engagement, but will that same model work well when they need to take on more clinical risk? Or are competitors better suited for that? What if plans only want to contract with people that know how to use upper case properly?
Conclusion + a few notes
I really enjoyed my ride along! As a newsletter writer, sometimes I feel very far divorced from how actual patients are impacted by things. This gave me a chance to talk to patients, see how they’re living, understand the environment, etc. Some last notes that I wanted to note about my trip:
- Wow my body can no longer do these day in, day out flights anymore. No one should have to see someone cut them in line using CLEAR twice in a 24 hour period.
- Living in New York, I take for granted how difficult not having a car is. You really can’t get anywhere around Memphis without a car and the public transit system is effectively non-existent. This is extremely limiting for patients - not only is it hard for them to get to appointments, but it’s hard even just having a social life or job.
- Housing is probably one of the biggest issues for SMI patients. Not only is there just not a ton of housing period, but SMI patients struggle to stay on good terms with roommates/landlords. This leads to a higher propensity for homelessness, which exacerbates the problem.
- The mental health of the peers themselves and caregivers who take care of SMI patients can really take a toll; they’re truly unsung heroes.
- Food deserts are very real. Grocery stores are literally miles apart while BBQ joints are on every other block. In fairness, you know which one of those my eyes were wandering to…

I chatted with one of the firsthand patients about his experience. He told me when firsthand reached out he was on his brother’s couch about to get kicked out and his schizophrenia was totally unmanaged. He truly viewed firsthand as a blessing from God. Several months later I was meeting him in his own apartment that firsthand found for him, with furniture that a firsthand peer helped find for him, talking about which medications were working well for him because he was actually going to the appointments.
I think the problem firsthand has set out to tackle is meaningful, difficult, and might be hard to scale. But it's clear that for the patients they work with, they can completely alter their life trajectories. And it’s hard not to root for that to work.
Thinkboi out,
Nikhil aka. "nikhil"
Twitter: @nikillinit
Other posts: outofpocket.health/posts
---
{{sub-form}}
If you’re enjoying the newsletter, do me a solid and shoot this over to a friend or healthcare slack channel and tell them to sign up. The line between unemployment and founder of a startup is traction and whether your parents believe you have a job.
Interlude - Apply to Knowledgefest! And healthcare 101 starts next week!
See All Courses →Don’t forget the application for our Knowledgefest, our healthcare software engineering conference IS LIVE.
If you work in healthcare ops, you want to be here. This is where you learn playbooks, see what other ops people are doing, and build your network. It’s year 5 and we sell out every year - applications are due end of month.
And if you feel like you really need to get up to speed on how healthcare works, then you should let me teach you at Healthcare 101starting next week!This is for anyone hiring teams of non-healthcare people that need to get up to speed quickly (in 2 weeks) - we do group discounts too hit up ya boy. You’ll even learn how to make memes.
.png)
Get Out-Of-Pocket in your email


