




How do we increase competition for hospitals?
Get Out-Of-Pocket in your email
Looking to hire the best talent in healthcare? Check out the OOP Talent Collective - where vetted candidates are looking for their next gig. Learn more here or check it out yourself.
 Hire from the Out-Of-Pocket talent collective
Hire from the Out-Of-Pocket talent collectiveFHIR 101

Featured Jobs
Finance Associate - Spark Advisors
- Spark Advisors helps seniors enroll in Medicare and understand their benefits by monitoring coverage, figuring out the right benefits, and deal with insurance issues. They're hiring a finance associate.
- firsthand is building technology and services to dramatically change the lives of those with serious mental illness who have fallen through the gaps in the safety net. They are hiring a data engineer to build first of its kind infrastructure to empower their peer-led care team.
- J2 Health brings together best in class data and purpose built software to enable healthcare organizations to optimize provider network performance. They're hiring a data scientist.
Looking for a job in health tech? Check out the other awesome healthcare jobs on the job board + give your preferences to get alerted to new postings.
Hospital prices going ALL THE WAY UP
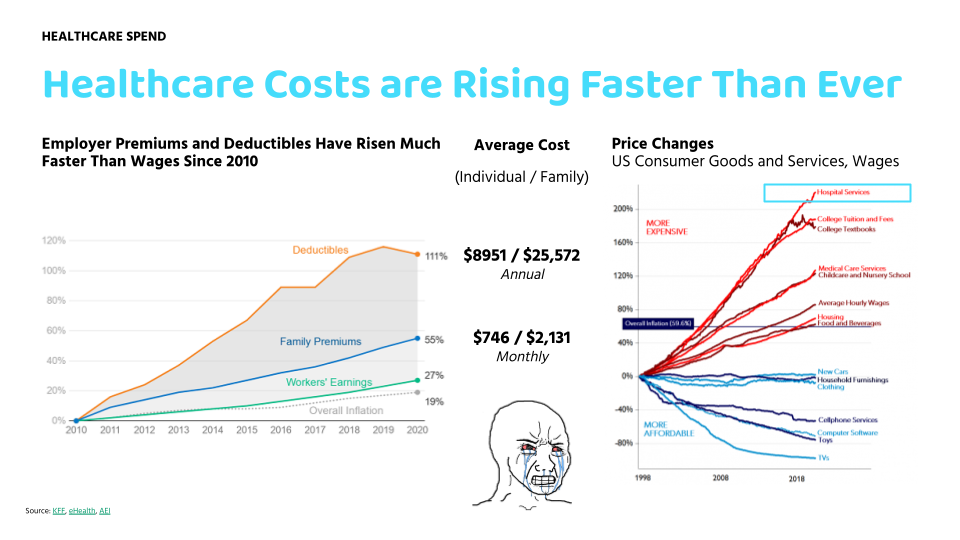
I feel very strongly that one of the missing pieces from healthcare is that we don’t have a competitive hospital environment. Hospital services have been one of the fastest inflating price buckets in the economy over the last few decades.
We go through this in the beginning of the healthcare 101 course (which starts 3/23!!! Sign up here if you or your team wants to actually understand how healthcare works).
Even college textbooks flattened out after they figured out PDFs and torrenting.
There’s lots of reasons people say why hospital prices have increased so much.
- Hospitals have consolidated massively over the last 15 years and bought up all the smaller group practices, so their leverage has gone up considerably in payer negotiations.
- More sites are considered part of the “hospital”. A lot of regular outpatient, same-day stuff will now get billed under the hospital umbrella which includes lots of extra charges.
- Commercial payers in particular are fragmented and each individual one lacks the ability to really negotiate down prices. Especially true when people are demanding a given hospital is in-network.
- Patients are getting sicker and more complex when they end up in the hospital so they need more things and the episodes get more expensive.
- Cause f*** it why not. What’re you gonna do, not go?
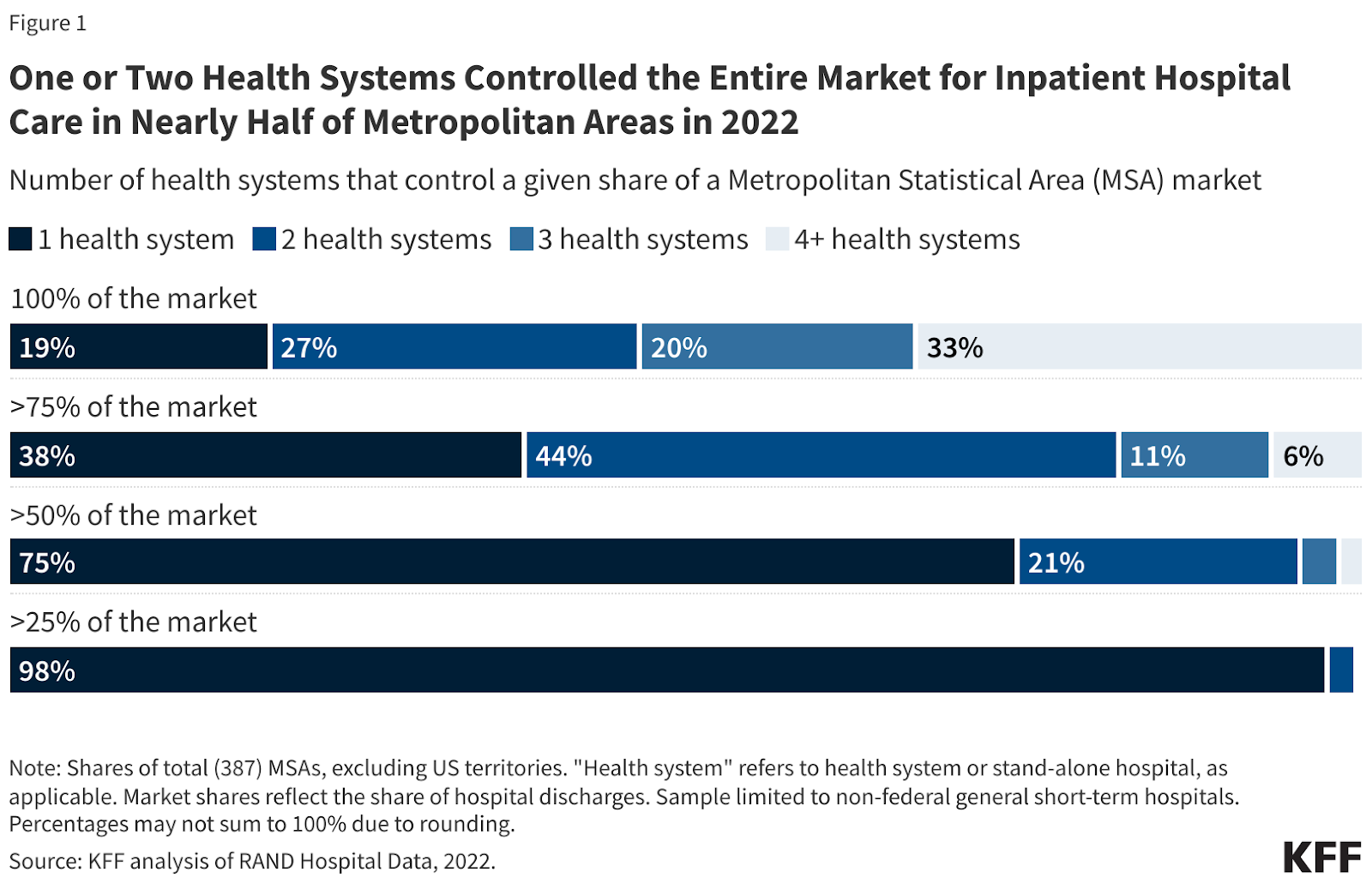
But IMO most of these are downstream from the basic issue that hospitals basically have no competition. If you look at most analyses for hospital concentration in a given area, you won’t be shocked to find that 1 or 2 of them control the bulk of the market in a given area.
So the question I have today is…how would you make the hospital landscape more competitive? IMO that means making more hospitals or letting non-hospitals do hospital things, but you might have a different read here.
Looking for practical suggestions, but also let’s get creative! I’ll put my favorite responses in the next newsletter.
Last call for hackathon applications!!!!
Applications for our healthcare hardware hackathon are due monday!! We got some baller judges like Julie Yoo (General Partner, a16z) and Tom Hale (CEO, Oura) and a secret third judge we’ll announce soon.
It’s going to be legit, you should apply even if you’re on the fence about it. You can learn more and sign up here.

And two more things
- Our Intro to revenue cycle management for digital health companies course starts next week! It’s FREE - if you’re a digital health company that needs to figure out how to bill you should come through.
- THE HEALTHCARE 101 CRASH COURSE IS OFFICIALLY OPEN FOR SIGNUPS! Starts 3/23, I’ll teach you everything you need to know about how US healthcare works. If you’re building here, selling into different entities, etc. you should take the course
{{interlude 3}}
Some small, practical changes we can make
There are certain regulatory tweaks that can be made that IMO would in aggregate have a big impact in making the hospital landscape more competitive.
Remove “Certificate of Need” laws - In many states, you need to get approval from the state before you build new facilities. These are called Certificate of Need (CON) laws. The general theory is that it prevents building duplicative services in a state and prevents providers from inducing care to use those facilities. Because once you build it, you’ll probably try to convince patients they need it.
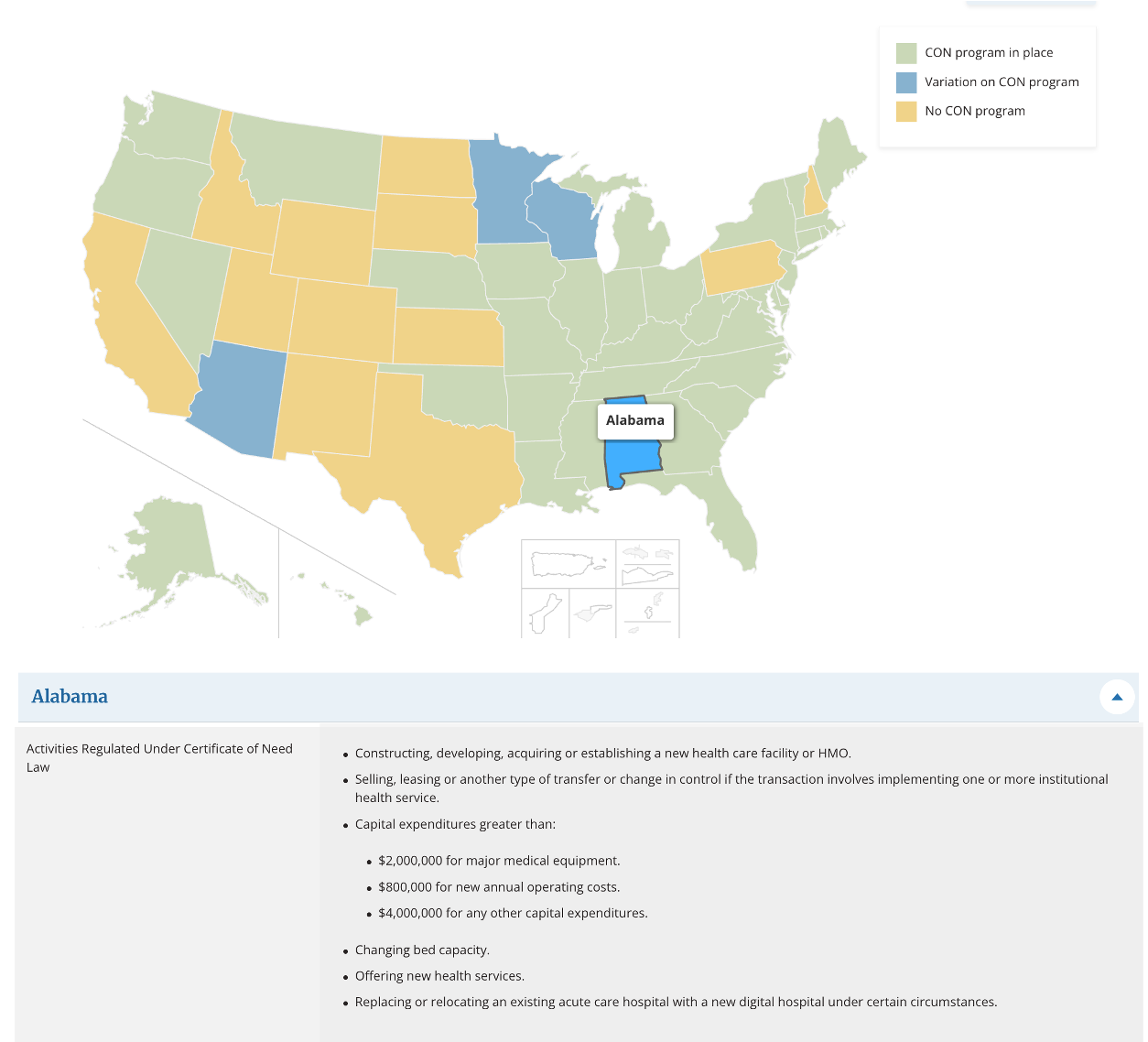
If you want more hospitals, we should make it easier to make new hospitals instead of needing to get permission from a committee each time. In the CON submission process competitors can make their case why a new hospital isn’t needed and can contest a decision to drag out the approval. In what world should competitors decide if you should exist?
All of this leads to increased uncertainty which also means the cost of getting capital to fund a new hospital becomes higher. For example Mission Hospital has been trying to prevent Adventhealth from building a new hospital in North Carolina for 3 years using the CON appeals process! This is pretty clearly bad for competition.
We should be PRO building more, not CON!!! Nikhil Krishnan for office.
Push site neutral payments - Today, Medicare will pay more for a service done in an outpatient setting if it’s owned by a hospital vs. an independent clinic doing the same exact service in the same setting. For example, a joint injection with ultrasound will cost ~$65 in a regular office vs. ~$327 if that same office is owned by a hospital. It’s like they slapped the Kith logo on the ultrasound.
The argument is that this boost in reimbursement is meant to cross subsidize the “money losing but societally positive” things that hospitals do. But I also think bad reimbursement structures like this are one of the reasons it’s hard to compete with hospitals. Plus it incentivizes hospitals to scoop up clinics so they can immediately juice the billing without changing too much.
The idea of “site neutral payments” means that the service will cost the same in those settings regardless of whether a hospital owns it or not.
Make non-competes unenforceable - This one seems like a layup, but I was also never good at layups. Lots of physicians have non-competes in their contract that prevent them from practicing in a given geography of their past employer. Given that you need clinical labor to create a new hospital or have any kind of competition, having non-competes seems bad!
The FTC was going to make a blanket version of no non-competes, but then pulled back from it. I think they should bring it back for clinical roles. Let them fight!
Allow physicians to own hospitals - CMS has effectively barred physicians from owning net-new hospitals. The idea was that if physicians owned hospitals, they were more likely to refer people for services they didn’t need or cherry pick patients with better insurance.
This is a much longer story and debate to be had. IMO at a high-level this:
1) Didn’t achieve the intended effect. The existing players like current hospitals and private equity still did all the things that people feared doctors owning hospitals would do since they have the same incentives but better lawyers.
2) Instead made more doctors employees of the hospitals and generally felt less agency in their roles. Your physician friend feels like an RVU monkey.
3) Reduced competition on the hospital side since physicians practically couldn’t start hospitals. It doesn’t help that many specialties want hospital-admitting privileges even if they wanted to have an independent group.
So making it possible and easier for physicians to own hospitals would introduce more competition to existing hospitals.
Enforce price transparency - We’ve had some pushes to make negotiated rates between hospitals and payers public, but there are many loopholes that have made it practically challenging to use that data.
If prices were clearer, we might also see more interesting plan designs that give patients $ to shop around between the different places of care and keep the dollars they don’t use. You see companies like Sidecar Health for example use plan designs like this.
Or more hospitals would compete and simplify their pricing if patients were using their own dollars. You see this in isolated slices like in Florida for cash pay patients where the price transparency regulations have more enforcement. Idk since it’s Florida I assume there’s probably some underlying crime that causes this though.
Bigger swing, “out there” changes
What about some crazier ideas on how to make new hospitals? The above are tweaks to make it possible to start new hospitals, but don't solve some of the other issues in actually running the hospital. In particular we need to solve:
- Physicians have a lot of debt and want stable money to suppor their lifestyles. So how do you attract them to work or start these hospitals? Also frankly they want prestige too.
- New hospitals need to get a flow of patients from somewhere.
- Payers give worse rates to new practices, hospitals, etc.
Some weirder ideas.
Employers banding together - I don't love how involved employers are in US healthcare, but a lot of hospitals were able to grow because employers helped front the bills or referred all their employees for care there (Kaiser, Noland, Ford).
Employers are feeling the pain of higher service costs and many are direct contracting with hospitals today. But a more interesting long term experiment could be whether local employers band together to help finance a new, lower cost hospital in a given area + create networks that heavily incentivize their employees to go to that hospital.
Standardized contracts - IMO one of the most underrated obstacles for new hospitals is the sheer complexity of payer contracting. It’s so complex and f***ed up, you have entire departments that need to handle this. If you know what “managed care contracting” is you need to find god.
I think it could be interesting if you had way more simplified and modular contracts, especially if everyone could see them. There are some interesting experiments happening here:
- Turquoise has Clear Contracts and Standard Service Packages to spin up simpler contracts powered by the price transparency data.
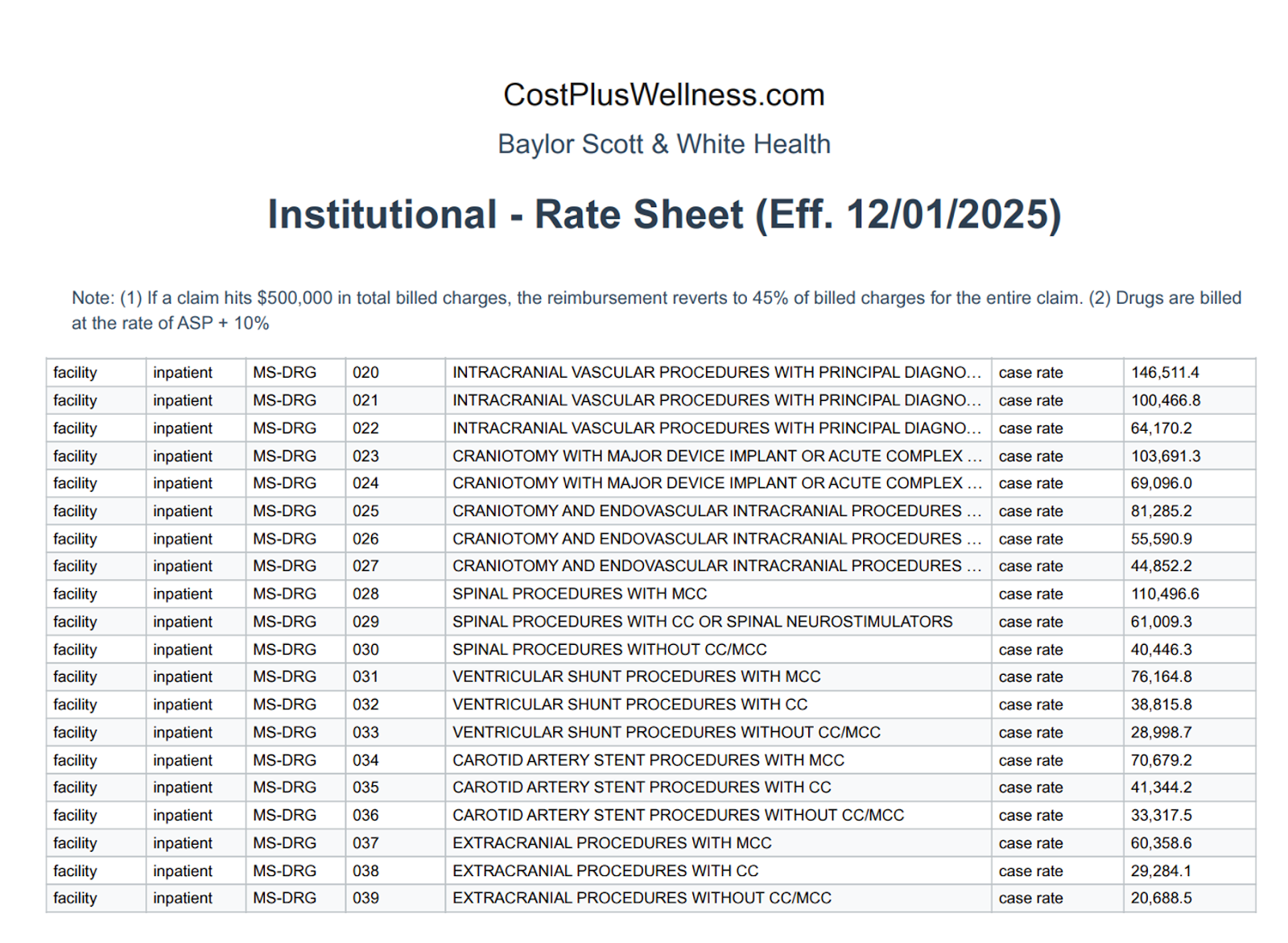
- Cost Plus Wellness has been publishing transparent contracts that they have with hospitals. There’s a big disclaimer at the top that says these are only meant to be used as a reference but…still interesting to see.
- CMS has something in the new LEAD model called CARA, an acronym matryoshka doll (CMS Administered Risk Arrangements). These are supposed to provide ACOs with shared data infrastructure, standard contract templates, and payment processing for specialist arrangements. What if CMS offered CARA-like infrastructure to new hospitals in concentrated markets? Provide standard contract frameworks, episode data, and payment rails that new entrants can plug into
Grants and bounties for doctors that start new practices/hospitals - Anecdotally when I talk to docs, there are a few different friction points when it comes to leaving existing hospitals or starting their own shop.
- You’d need a group of docs to leave together. This is both to be able to get referrals but also so that there’s more coverage for each other. And they need coworkers to shit talk, that’s like half the fun of a job.
- The costs are high to start and all of the doctors either have debt or relatively cushy salaries with 2 kids in private school with esoteric and expensive hobbies.
- A lot of the stuff we talked about already (CON laws, bad insurance reimbursement until you hit volume, non-competes, not allowing docs to own hospitals, etc.)
The first two points feel like an issue money could help solve. What if there were grants for doctors to go start new hospitals? This might help defray the upfront costs and smoothen out the salary shock a bit more. You’d probably have to tie it to hitting some level of patient volume in a certain amount of time so that people don’t just start hospitals to get the money. Or maybe you could do something like a loan forgiveness program for doctors who start new hospitals/practice in areas that lack competition.
One version of this might just be extending CMMI’s AHEAD model. This model gives hospitals prospective global budgets rather than fee-for-service payments. Basically this means a hospital gets a predictable annual revenue amount based on their patient population. The hospital gets revenue stability in lieu of potentially higher but more fluctuating payments.
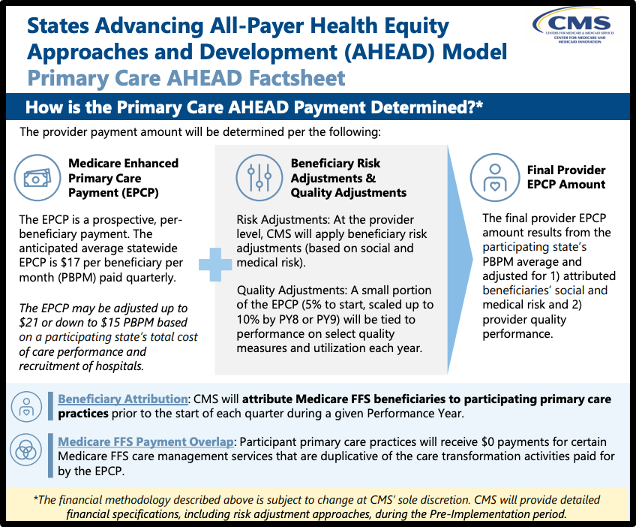
Maybe you could extend these AHEAD-style global budgets specifically to new hospitals in highly concentrated markets. Groups of doctors could apply together to get funding. An interesting byproduct could be new, AI-native hospitals that actually manage to significantly lower their operating expenses to make margin underneath that fixed budget?? I’m getting AHEAD of myself.
Just spitballin’ here, but we need to find a way to get individual docs excited about the idea of starting their own hospitals (if they’re allowed to). Money makes anyone a little bit more excited, doctors aren’t special.
Enable more microhospitals - A few companies like Nutex, Emerus, etc. are building hospitals with way smaller footprints. These are hospitals that are a fraction of the size, 6-8 beds + inpatient beds, specialists on call and virtual, and have the tools to stabilize and fast track emergency patients. You can see a list of examples here.
I do think there’s something interesting about using microhospitals + hospital-at-home to create what effectively look like hub-and-spoke hospitals. The footprint and cost is way lower and you can deploy them into underserved and rural areas. Technology should also theoretically make it easier to have a specialist in your pocket + smaller tools to monitor patients at home. And it’d be cool to have roommates again for a bit, even if that roommate is giving me a nebulizer.

Celebrity or Company hospitals??? - Instead of really rich people donating for another cancer wing of a hospital, I think it could be interesting to fund a new community hospital. Hospitals are pretty bad businesses but celebrities love donating to questionable non-profits for tax optimization and good vibes. Let’s use non-profit designation for hospitals to our advantage.
At the end of the day one of the reasons people want brand name hospitals in-network is because those hospitals have brand recognition for being good. What if a celebrity gave their brand recognition to a new hospital. Idk man people are weird and might prefer to go to a Mr. Beast hospital vs. Cleveland Clinic. Ohio is literally a slur for Gen Z.
Or maybe it would be a company with a specific type of brand association - e.g. a Costco hospital that charges a membership and everything is at cost. I mean…the Costco hot dog is still $1.50, you don’t see that on the price inflation chart.
Listen, no such thing as dumb ideas in a brainstorm right?

OOP Healthcare Coworking
By the way, if you’re looking for a coworking space and want to be around other healthcare people…
We run coworking spaces in Chicago, SF, New York, and Boston and currently have 80+ people across them. It’s a good time, come through.

Conclusion and parting thoughts
One big thing to consider with all of the things above is whether changing these rules will simply allow existing hospitals to build new facilities, extend their footprint, and gain even more leverage than they already have. Or whether people would exploit these rules to do crazy billing schemes on patients that end up in the hospital in an emergency.
The second is to make sure that there’s some form of auditing that can happen to make sure that increasing hospital competition doesn’t also push those hospitals to also cut down on quality in egregious ways. For example, physicians self-referring risky procedures because they own their own facilities.
I’m sure there are lots of tradeoffs we’d be making with some of my suggestions, but I figured I would get the conversation started.
Give me your suggestions, how would you make the hospital landscape more competitive or bring prices down? I’ll put my favorite answers in the next newsletter. Please give me answers that are more creative than “the government should decide the prices”. Or even better, if you disagree with the entire premise tell me why!
Thinkboi out,
Nikhil aka. “Hospital YIMBY” aka. “Beast Games: Hospital Edition”
Twitter: @nikillinit
IG: @outofpockethealth
Other posts: outofpocket.health/posts
If you’re enjoying the newsletter, do me a solid and shoot this over to a friend or healthcare slack channel and tell them to sign up. The line between unemployment and founder of a startup is traction and whether your parents believe you have a job.
Quick Interlude - NEW COURSE ON FHIR! KNOWLEDGEFEST APPS DUE SOON!
See All Courses →So...what actually is FHIR? I get this question a lot, but there's never really enough time to explain it and also I would just mumble "technical standard" and walk away.
So we decided to do a standalone free FHIR 101 course in partnership with Redox! Over 3 days in August we'll go over the spec itself, how it differs from other healthcare information standards, and practical tips to build with it.
I wanted to call it FHIR fest but it got nixed. You can sign up for it here, it's FREE and it's 8/25-8/27.

And a reminder that Knowledgefest apps are due this week. If you want to be in a room with the best ops people in healthcare, you should apply like TODAY.
We sell this conference out every year - all workshops, learn how people are building and scaling in healthcare, application based so we only take the best. We have people from Commure, Clarity Pediatrics, Pomelo, and Waymark already coming, join the squad.

Get Out-Of-Pocket in your email


