




uBiome - how microbiome testing becomes fraud
Get Out-Of-Pocket in your email
Looking to hire the best talent in healthcare? Check out the OOP Talent Collective - where vetted candidates are looking for their next gig. Learn more here or check it out yourself.
 Hire from the Out-Of-Pocket talent collective
Hire from the Out-Of-Pocket talent collectiveHealthcare 101 Crash Course
%2520(1).gif)
Featured Jobs
Finance Associate - Spark Advisors
- Spark Advisors helps seniors enroll in Medicare and understand their benefits by monitoring coverage, figuring out the right benefits, and deal with insurance issues. They're hiring a finance associate.
- firsthand is building technology and services to dramatically change the lives of those with serious mental illness who have fallen through the gaps in the safety net. They are hiring a data engineer to build first of its kind infrastructure to empower their peer-led care team.
- J2 Health brings together best in class data and purpose built software to enable healthcare organizations to optimize provider network performance. They're hiring a data scientist.
Looking for a job in health tech? Check out the other awesome healthcare jobs on the job board + give your preferences to get alerted to new postings.
Flashback - uBiome of Microbiome Testing Infamy
There’s a lot of fraud that goes on in healthcare. It’s the perfect blend of a gigantic amount of money, a lot of patients who are desperate and looking for guidance, and transaction webs so complicated it makes Tenet look understandable. This is a scammer’s paradise.
But also, fraud cases are one of the few times we as outsiders get clued in on the mechanics of how a lot of healthcare works via the investigations, even if it’s in a distorted way. So, I’m going to try and go through some fraud cases and use them to explain some parts of healthcare.
Let’s start with uBiome. uBiome was a company that provided microbiome testing and sequencing. There were a million different 23andMe for X’s that popped up in the mid 2010s. 23andMe for dogs, 23andMe for weed, so 23andMe for dat ass was inevitable.
uBiome had 3 products:
- Explorer - a direct-to-consumer kit (under $100). You mailed a stool sample, the lab sequenced the microbiome and gave you a comparison report versus other users. It was not marketed as diagnostic and wasn’t billed to insurance.
- SmartGut — the “clinical” version of the gut test. It identified microbes from a fecal sample, was positioned for clinician use, and attempted to get insurance reimbursement.
- SmartJane — a vaginal microbiome clinical test; also billed to insurers.
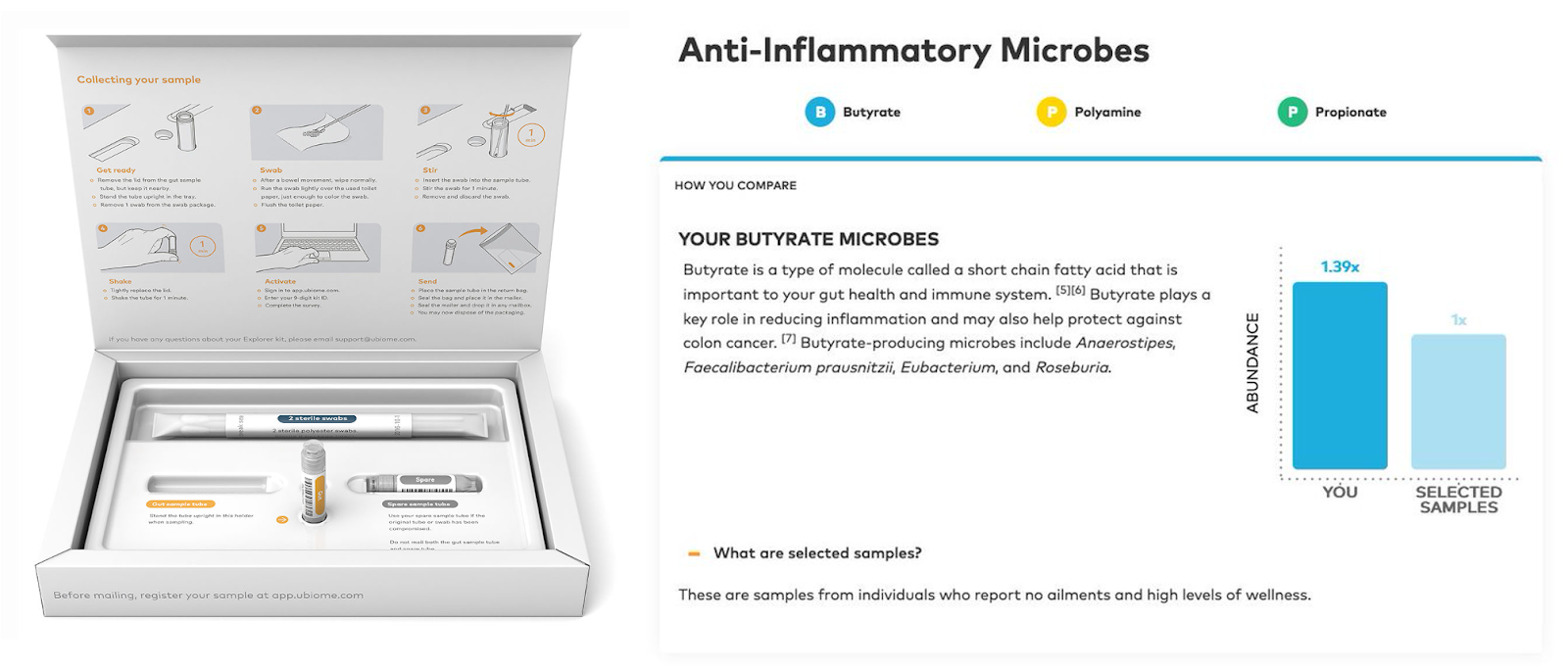
At a high level, the company had a product that could test shit (literally). The problem was that it’s hard to build a big business in direct-to-consumer testing, so they wanted to get reimbursed by insurance.
*disc scratch* And that’s where the troubles began.
[I think I need to say this all happened allegedly. This is according to the indictment and the Wall Street Journal reporting. So uh, this is alleged and please don’t sue me?]
Quick Context - Lab Developed Tests and Billing Insurance
Let me explain some important context on how things normally work.
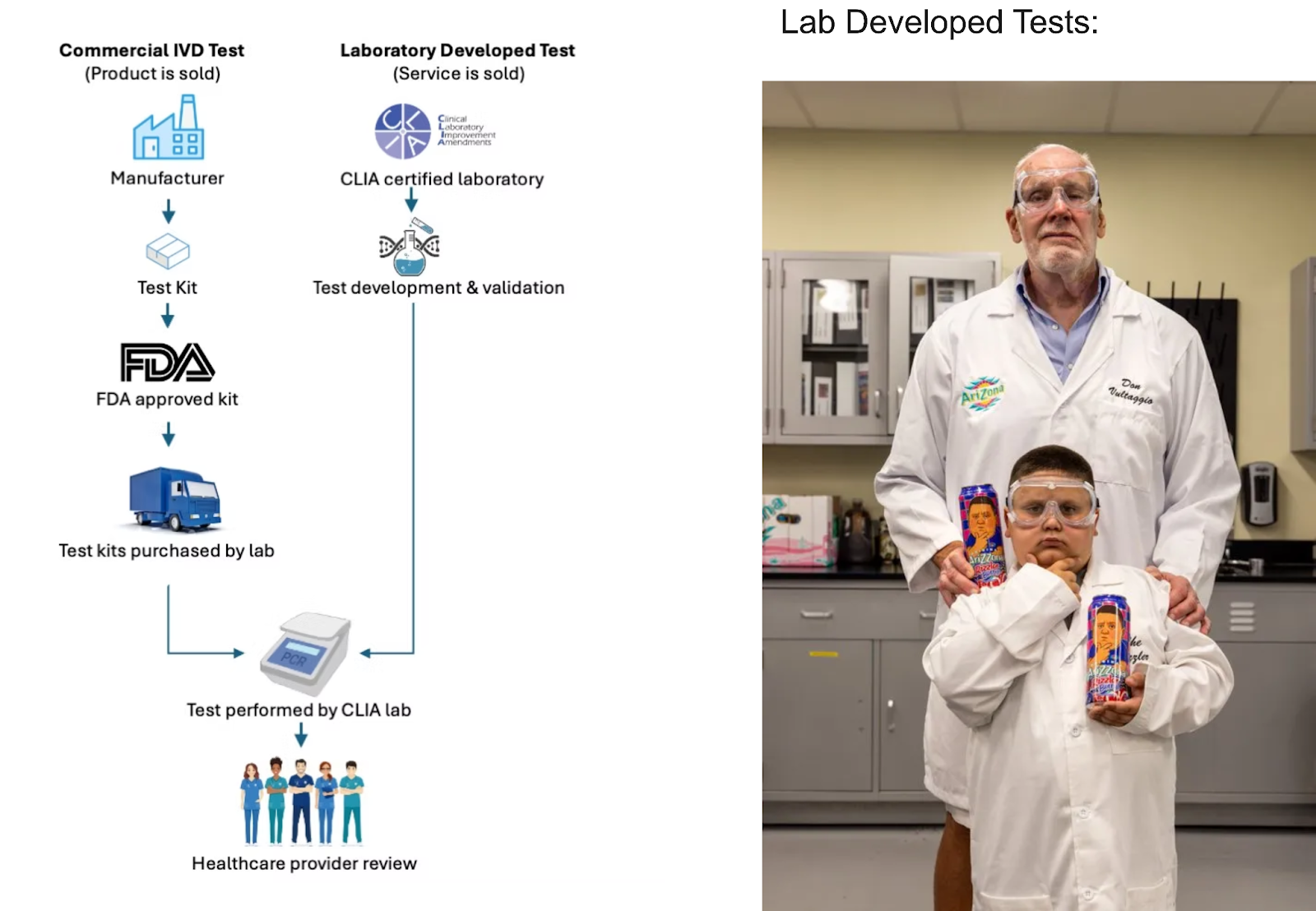
A test doesn’t necessarily need to go through the FDA. “Lab Developed Tests” (LDTs) can be developed and validated from any lab with a CLIA certification (usually for high-complexity testing). The idea here is that clinicians and patients can trust these tests because they were developed by a lab that has CLIA's stamp of approval.
A classic example is an in-house molecular oncology panel to genetically characterize tumors. Hospital X's pathology lab can build and validate it in house, but it can't be used by any other hospital without FDA clearance, which is highly burdensome to obtain.
The catch is that LDTs can only be run in the labs that developed them. And those labs also can’t market it as an FDA approved test (which especially matters to physicians) and it’s usually a fight to get these kinds of labs approved by insurance.
It can be faster and cheaper to get your tests in the hands of patients via LDTs and later go through the FDA route when you want to scale, get payer reimbursement, etc.
Second, here’s what the normal flow would look like as a patient.
- I see the doctor, they think this Lab Developed Test would be useful for me. They check against the insurance guidelines to see how they determine if this could be medically necessary and if they’ll reimburse it.
- The lab sends a bill to the insurance company under a CPT code that makes sense. For example, there are catch all codes like 81479 (Unlisted molecular pathology procedure) that it would make sense to bill your test under.
- The insurance company might ask for some justification and documentation on why this test is needed. They want to see that the test is going to change care in some way and might require other tests first.
- The insurance company approves the test and reimburses the doctor a certain amount. The lab then has to get the copay, coinsurance, or amount under the deductible from the patient. (Sometimes, the copay is charged upfront when the test is ordered).
This feels doable assuming that your test is something that insurance believes falls into clinical guidelines and docs would order to guide their treatment. But…hypothetically, what if you had a test that wasn’t like that?
{{interlude 3}}
What Made uBiome Fraudulent?
uBiome unfortunately did not have a test that payers really wanted to reimburse. It provided some interesting things for patients to explore about their microbiome, but it wasn’t clear that this test was medically necessary or actually changed the course of care for a patient.
But going to direct-to-consumer is a way smaller business than getting insurance to pay for it. So how do you get insurance reimbursements for them if you don’t have a clinically useful test?
Well, there are a few things that put it in the cross hairs of a criminal case.
Quick note: Final 3 courses this year + last call for Boston coworking
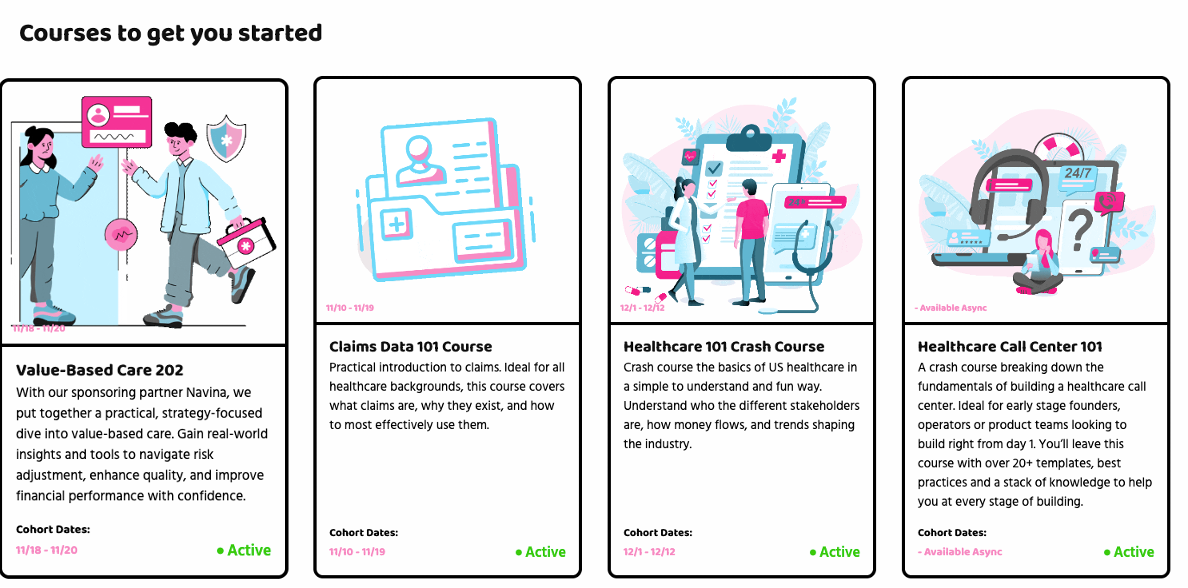
We’re running three final courses this year
- Claims Data 101 (starts 11/10) - Claims, the great morass of billing data that gets used for all sorts of non-billing stuff. We’ll explain how claims are made, weird quirks when analyzing them, and real-life examples you’ll run into. This is the final run of the course!!!
- Value-Based Care 202 (FREE, starts 11/18) - We’re partnering with Navina to talk about what quality scores are, ops in value-based care, and how AI is making it all fun and different today. It’s free, come through!
- Healthcare 101 (starts 12/1) - Instructor is super charismatic, he’ll teach you everything you need to know about US healthcare quickly. The laws, how money flows, what a PBM is, what an “integration” is, and more. Come hang!!
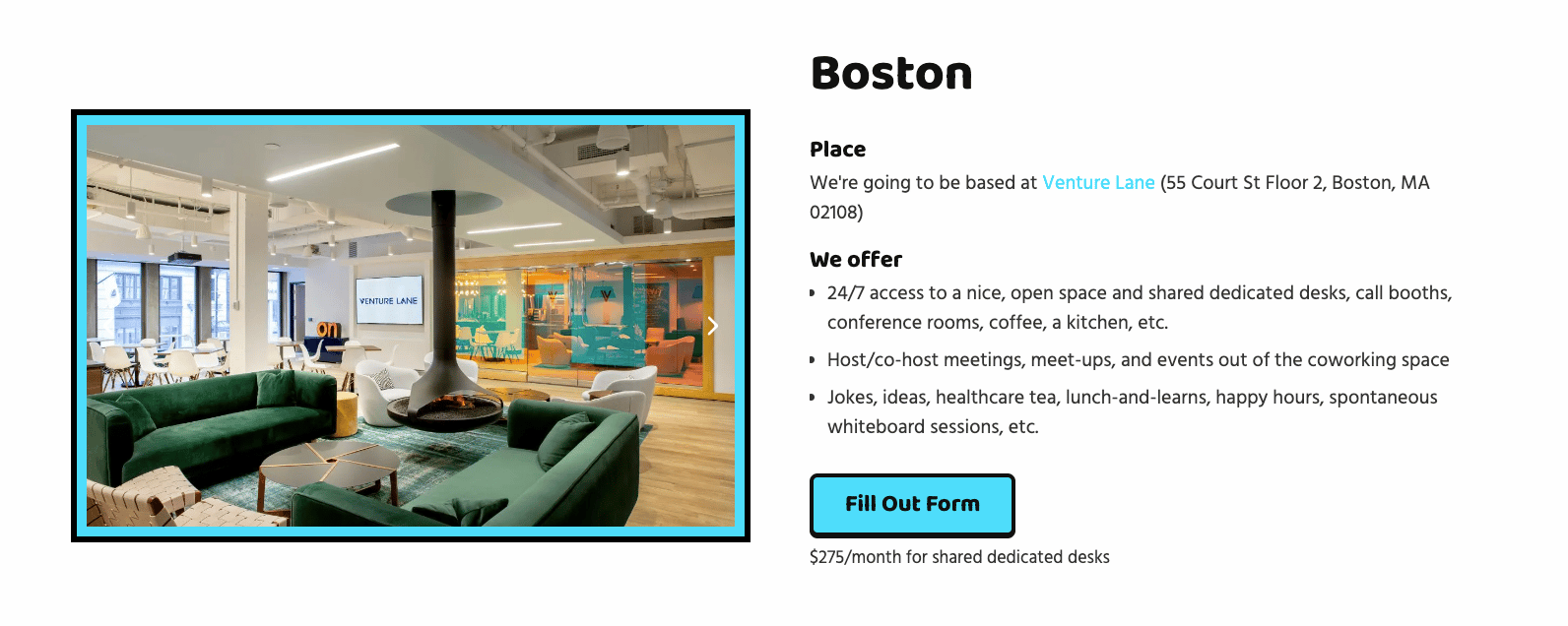
Also, LAST CALL TO JOIN OUR BOSTON HEALTHCARE COWORKING SPACE. We're getting a group of healthcare people together to cowork together because remote work is isolating!!! We'll get the group together for happy hours, some talks, etc.
We have a limited number of spaces - so if you're interested would let us know ASAP by filling out this form.
“Upgrades” of Archived Samples
When uBiome had new tests, one thing they’d do is run those tests against old specimens that patients had sent in. Where they had this locker full of old stool is not something I really want to know the answer to.
It doesn’t really make sense to run a new test against an old sample since we don’t know if the patient’s health and microbiome have changed. Payers generally view repeat testing as non-covered unless there’s a new clinical question that can be answered. For a microbiome that’s constantly changing, you’d want to use it on a new sample for it to be clinically relevant.
But if you lack a moral compass, then you can run those tests on anything you want. uBiome would do this and bill payers, which essentially allowed them to bill stupid amounts per patient. They even marketed to patients that they could “upgrade” their tests on all their old samples with one click.
Internal emails referred to this as a “growth hack”, which is definitely one way of saying it. But if you’re doing it, it’s not medically necessary, and if you bill Medicare, it’s gonna be fraud.
Doctor-Ordered Through a Contracted Physician Network
Normally, these Lab Developed Tests get ordered organically from clinicians that patients are already seeing. But, that’s much slower since patients are getting sent in one provider at a time.
Instead, uBiome created a third-party network of contracted doctors that often didn’t have a real visit or full history and sort of rubber stamped the test as medically necessary if patients requested it. And since those doctors didn’t actually have a relationship with the patients, that makes “medical necessity” hard to justify. Especially since those docs aren’t changing any treatments for the patients since they aren’t ACTUALLY their patients.
On top of that, uBiome purposefully withheld info from these docs about whether the tests ordered were these “upgrade” tests on old specimens. So doctors were approving tests without knowing the full context.
When insurance asked for further documentation, uBiome would create fake documents about the patient-provider interaction and submit it as if the doctor had actually done those things. Writing fake doctor’s notes is reserved for sophomores getting out of the Orgo midterm (and going on to write newsletters).
Waiving the Patient Copays/Deductibles
Payers have things like copays and deductibles so that patients have some skin in the game and won’t get unnecessary medical stuff. Because of that, a doctor also can’t just say “hey, we’ll forget to collect your copay if you get this service hint hint wink wink”.
uBiome did exactly that. Not only would they routinely waive copays and coinsurance from patients by saying they were in a “pilot program where uBiome will cover all the costs”, but they would even do things like give gift cards if patients actually mailed their samples back. Not only were they not collecting money from patients, they were actually inducing them to get tests done by paying them.

Getting your own stool sample is one of the nastiest things in the world and there aren’t enough gift cards to remove the olfactory trauma.
[It’s worth noting that there ARE legal ways to set up a patient assistance program, and if you’re interested in this you should talk to a legal team that specializes in this. But at a high level you need to have strict criteria on what patients fall into this category and actually document it, not blanket approve everyone.]
Billing Shenanigans Around Dates
At a certain point you have to be like f*** it, just full send billing fraud let’s rip it.
uBiome would change the dates of services that they billed insurance. This allowed them to bill after a patient’s deductible was met, which meant the patient was more likely to get the test fully covered.
They also sent bills to insurance as a lab developed test before they even got their CLIA certification in order to show investors that they could bill insurance. Obvi, can’t do that.
And finally, they would A/B test which CPT codes to bill under just to see which ones would get approved vs flagged. Most of the time they billed 87507, but would change it up for upgrade so that insurance would suspect the same test was being run. Generally, you’re supposed to bill consistently if it’s the same lab test, so this is a red flag.
Other Tidbits Around this Lawsuit
The lawsuit had some other interesting factoids in it.
The craziest part is that once this whole thing started unraveling in 2019, the two co-founders Jessica Richman and Zachary Apte got married to each other and then fled to Germany where they’re currently fugitives!! What??? Germany is not a country that extradites citizens to the US, and Zachary Apte was a citizen. It’s so embarrassing that they got away with this! And if they’re reading the newsletter, shame on you but also don’t unsubscribe. I can’t afford it.
Second is that you can see how much the founders personally sold in the fundraises while this was going on. The Series B (which seems to have been $22M total) allowed the founders to sell $1.2M of their own shares each. In the Series C they sold $5M each in a $83M fundraise. In total that meant that founders each got about ~$6M through this each. Don’t know how ya’ll do that 9-5 grind 😤.
Last and most hilariously:
“To stoke press interest and to obtain press coverage of uBiome, which press coverage could then be distributed to investors, APTE and RICHMAN led others to believe that RICHMAN was younger than she was. For example, in or about June 2015, RICHMAN stated in an email to a reporter who was writing an article about RICHMAN that she was “under 40,” when in truth she was not.
RICHMAN later included a reference to the article on her resume and included a link to the article on uBiome’s web site and in materials that RICHMAN intended and knew would be received by investors.”
Lmaooooooo. I mean honestly I blame tech culture for putting this weird idea into the universe that being accomplished under a certain age is better. If you’re someone who thinks it matters to be on an “under 30” or “under 40” list, you are a sheep that deserves algorithm slop.
The only thing more embarrassing than being impressed by someone on an under 40 list is lying about your age to get on it.

Some Idle Thoughts Around this Case
I condemn this, I think it’s bad, yada yada yada disclaimers to make sure it doesn’t seem like I’m downplaying the significance of all this. But a few things popped into my head as I looked more into this case.
- There’s an open question around whether direct-to-consumer diagnostics is something we need as a society. A big part of this case is about how uBiome marketed to consumers that they could get all of these things tested for when there really isn’t much clinical evidence to back that up. Especially in an area where there aren’t a lot of options for patients (e.g. people suffering from gastro issues), it does feel like it can be predatory. On the flipside, I also think patients should have more agency in their healthcare decision making and diagnostics are one of the best ways to do that.
- There’s been a big fight over when it’s okay for companies to use contracted out doctors that loan their license to put in orders. I think there are a lot of things we make unnecessarily difficult to get and it really is a commodity transaction (e.g. simple med refills, basic labs, etc.). Maybe docs don’t need longitudinal relationships with patients for these encounters and this increases access for patients. On the other hand, this case shows the more extreme examples where a lot of the docs just don’t really care what’s happening, get paid, and don’t question things like medical necessity.
- uBiome billed $300M to insurance but only got paid $35M. Does that look good or bad for insurance if only <12% of these actually managed to go through?
- This is a good example of why you should actually dig into the accounts receivable if a startup has a big delta between what they are contracted and what they’re actually getting into the bank.
- Interestingly, a lot of these claims were brought to the attention of California state agencies and journalists because one of their customers basically looked up how they bill CPT codes and then made a dossier of why he thought it was fraud. There is nothing more dangerous than a customer with a vendetta and time on their hands.
“Damian Moskovitz: I spent literally scores, if not hundreds of hours, going through reams of paperwork, insurance documents, everything I could find on uBiome's website, related scientific information, making spreadsheets.
Amy Dockser Marcus: What made you so curious? It's like a lot of labor that you put into this.
Damian Moskovitz: So in short, I have a strong sense of justice and I dislike waste and I dislike high health insurance costs. And I was angry when I started to realize that this house was made of cards. They're offering a test that they argue is medically sound and therefore reimbursable by insurance companies and gives people like myself hope of successful treatment for a debilitating condition. To find out that none of that is true was very upsetting to me. It gave me a lot of false hope and it was a big waste of my time.” - Wall Street Journal
This dude saved the healthcare system more money than the average value-based care company just by being vindictive af. I love it.
Featured job postings!
Some companies are hiring, check them out!!!
Joyful Health - Strategy & Operations Lead or CoS (NY)
- Joyful Health is building an AI financial OS for healthcare. As our first business hire, you’ll lead operations and scale our first product line. This is a leadership role with significant autonomy. Experience in healthcare ops & IB/finance is helpful.
Amperos Health - Product Manager, Agents (NY)
- We're building the AI workforce for healthcare RCM. We're looking for a great product manager to own new AI product surfaces. These agentic products might span across voice AI, browser agents, clearinghouse APIs, etc. Come build at the frontier of healthcare and AI with us.
Daymark Health - Director of People Operations (Boston, NY, Philly)
- Architect the people systems that power Daymark’s mission-driven cancer care model. Build scalable hiring, performance, and engagement programs as we grow nationwide. Join us in transforming oncology care.
Yuzu - Operations Architect (Legal)
- Yuzu is a health insurance administrator powering innovative health plans (covering 15k+ members). We have a strong "do-it-in-house" culture and are excited about bringing on a first employee to manage legal product and operations work reporting directly to Russell
Conclusion
Again, all of this is allegedly or whatever gets me out of legal trouble. Bye.
Thinkboi out,
Nikhil aka. “when shit hits the fan” aka. “Theranus”
Thanks to Sanjat Kanjilal for reading drafts of this
Twitter: @nikillinit
IG: @outofpockethealth
Other posts: outofpocket.health/posts
{{sub-form}}
If you’re enjoying the newsletter, do me a solid and shoot this over to a friend or healthcare slack channel and tell them to sign up. The line between unemployment and founder of a startup is traction and whether your parents believe you have a job.
Interlude - Apply to Knowledgefest! And healthcare 101 starts next week!
See All Courses →Don’t forget the application for our Knowledgefest, our healthcare software engineering conference IS LIVE.
If you work in healthcare ops, you want to be here. This is where you learn playbooks, see what other ops people are doing, and build your network. It’s year 5 and we sell out every year - applications are due end of month.
And if you feel like you really need to get up to speed on how healthcare works, then you should let me teach you at Healthcare 101starting next week!This is for anyone hiring teams of non-healthcare people that need to get up to speed quickly (in 2 weeks) - we do group discounts too hit up ya boy. You’ll even learn how to make memes.
.png)
Get Out-Of-Pocket in your email


