




The Impact Of Self-Driving Cars On Healthcare
Get Out-Of-Pocket in your email
Looking to hire the best talent in healthcare? Check out the OOP Talent Collective - where vetted candidates are looking for their next gig. Learn more here or check it out yourself.
 Hire from the Out-Of-Pocket talent collective
Hire from the Out-Of-Pocket talent collectiveHealthcare 101 Crash Course
%2520(1).gif)
Featured Jobs
Finance Associate - Spark Advisors
- Spark Advisors helps seniors enroll in Medicare and understand their benefits by monitoring coverage, figuring out the right benefits, and deal with insurance issues. They're hiring a finance associate.
- firsthand is building technology and services to dramatically change the lives of those with serious mental illness who have fallen through the gaps in the safety net. They are hiring a data engineer to build first of its kind infrastructure to empower their peer-led care team.
- J2 Health brings together best in class data and purpose built software to enable healthcare organizations to optimize provider network performance. They're hiring a data scientist.
Looking for a job in health tech? Check out the other awesome healthcare jobs on the job board + give your preferences to get alerted to new postings.
The Church of Waymo
The first time I got into a Waymo in SF I legit had a spiritual experience. This cityboi had just gotten his driver’s license for the first time, and I felt like the last person who chose horse carriage driver as a career.
Getting in that car was one of the few times I had a visceral reaction to technology, knowing I had really just peeked at the future. I was edging as I saw it handle edge cases.
Of all AI use cases, I think self-driving cars are going to have one of the largest effects in the US. Our entire society is shaped around cars, the second order effects of making them driverless are still understudied.
I thought I’d do a little bit of a thought experiment on what some second-order effects of driverless cars might be in healthcare. If you have other interesting thoughts here, send them in.
HEALTHCARE 101 LEARNING SUMMIT - REGISTRATION CLOSES 1/21
Final call here!!!! If you or your employees need to get up to speed quickly on healthcare, join us in NY 1/29-1/30 for the healthcare 101 learning summit. We’ll teach you the basics, the trends, you’ll meet some awesome people.
Email sales@outofpocket.health for group rates. ENROLLMENT ENDS 1/21!!!! Sign up here.

Next week is our FREE course on interoperability. With the announcement of ChatGPT health and OpenAI for Healthcare, all the conversation has been about using LLMs to analyze healthcare data. But how do you GET all the contextual data needed to make those analyses good?
In our course with Metriport starting next week - we’ll go over how to pull healthcare data into applications and what’s happening with new regulations. Even if you can’t make it, sign up to get the slides and recording.

Fewer Crashes and the Second-Order Effects
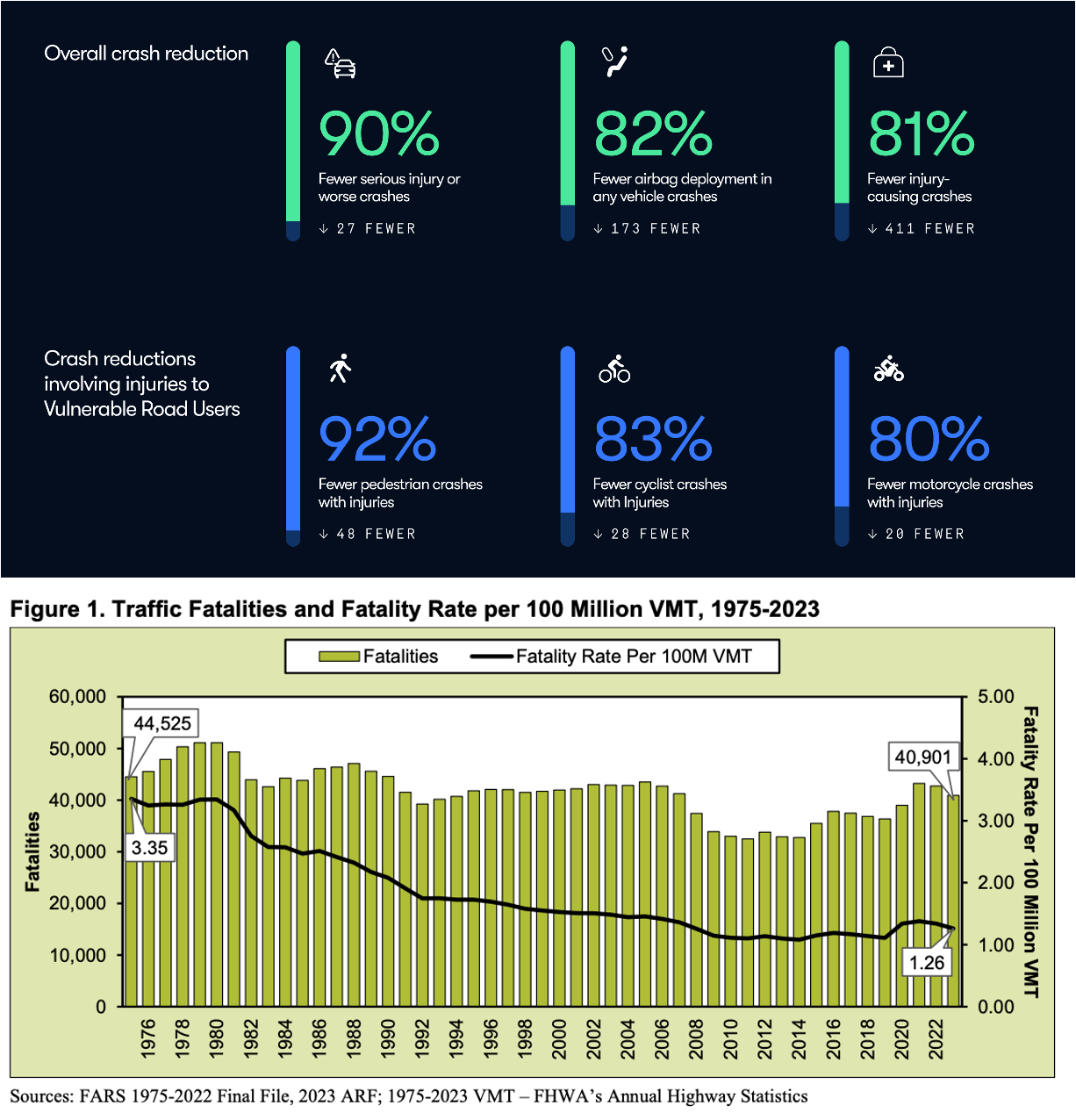
According to the NHTSA, there were about ~41K motor vehicle deaths in 2024. 30% of those were due to drunk driving. Another ~1.7M crashes caused an injury.
When you look at Waymo’s safety data, there’s a 90% drop in crashes causing a serious injury or fatality. Yes this is in a smaller number of cities and they currently operate in low speed zones, but it’s clear that this is going to significantly reduce the number of auto deaths, which is great.
What does it mean for the healthcare system if there are fewer auto crashes? Other than Subaru drivers needing a new hobby:
Trauma units will see their economics and case mix change - Inpatient trauma care is about 25% of all inpatient costs. Within inpatient trauma care, motor vehicle accidents are about 22% of those costs, though only 14.5% of visits. If this drops, trauma units will be mostly old people, falls, and Medicare. The number of trauma units + where you’d place them will probably change, too.
Less motor vehicle injury rehabilitation will be needed - For long-term inpatient stays that require rehab, two of the buckets are traumatic brain injury (TBI) and traumatic spinal cord injury where motor vehicle accidents are in the top two causes. The rehab for moderate-to-severe versions of these injuries tend to cluster at providers that specialize in these (e.g. TBI specific hospitals). For example, in this study of multiple TBI specific sites, 56% of total patients were from motor vehicle accidents.
Providers that focus on specific types of care downstream of motor vehicle accidents will probably need to either shift to a different specialization, or expand to other rehab types.
This will exacerbate an organ shortage - More than 10% of all kidney donations came from auto crashes in 2023. We’re already in an organ shortage; this is likely going to make the situation worse. We’re going to need artificial organs or xenotransplantation to come faster. Some of you have been on the waitlist for a brain transplant for too long.

Do payers get a benefit? - I wanted to see how much money payers would save thanks to self-driving cars. This paper sort of answered it for me. Medicare would save about $4.2B (~0.5% of total spend) and Medicaid would save $6B (~1% of total spend). Private insurance is harder to figure out because workers comp, auto, and commercial insurance are bundled together, and that requires actual work to figure out.
I was surprised at the self-pay and uninsured stats, which would be ~$3B saved. No insurance (self-pay and charity care) represent 12.5% of motor vehicle accidents that end up in the emergency department, which is a lot relative to the amount spent. I’m curious if anyone has a sense of why this is.
All in all, it doesn’t really seem like that much savings for payers, and that spend will likely end up showing up in increased prices elsewhere.

{{interlude 3}}
Making it Easier to Move People + Work in the Car
When thinking about driverless cars, the most immediate place your mind might turn is non-emergency medical transport. This is basically moving patients from a doctor’s office or hospital back home and vice versa but they wanted to call it something fancy so they can charge more. If a patient is getting discharged post-surgery, or otherwise has a mobility issue, they’ll need a car (potentially with modifications) to take them around.
Depending on which source you look at, somewhere between 2-5% of people don't get medical care in a given year because of transportation issues. Rideshare can address some of these problems; it’s why Uber and Lyft have their own healthcare programs. Self-driving cars could bring those costs down or make care more accessible in areas where there are less drivers.
But a more interesting dimension is looking at what’s possible if you don’t need to pay attention to the road or if there’s no one else in the car with you. This is where we can start getting into the weirder ideas.
Telemedicine cars - Many healthcare companies have some concept of “windshield time”, which is time that their staff need to drive from place to place. This could be driving between patient’s homes, doctors driving between sites of care, etc. This is considered dead time and becomes a real consideration especially when you get to more geographic sprawl.
If there’s no driver in the car, the car itself actually becomes a secure place to have healthcare interactions. What used to be dead time could conceivably now be time for doctors to do telemedicine visits, second opinions, adjust and edit notes, etc. Honestly, you don’t need to change anything about the current self-driving cars for patients to start using their phone for telemedicine visits today, technically.
Sleeper cars - If cars don’t need drivers, you can presumably re-design them for different interiors. One version of this will likely be cars with beds that allow you to sleep in the car while it brings you to a destination. This raises three questions.
- Will patients be willing to travel further for care that’s better? Getting on a plane to get care is a huge friction, but maybe sleeping in a car isn’t as big of a deal if it means you wake up somewhere where their care is better.
- Will clinicians be more willing to travel to work? Most clinicians now want to live in places that are more population dense, but patients need care in more rural areas. Maybe health systems use sleeper cars to send docs to more rural areas, do a shift in the area, and then have a sleeper car bring them back? It’s also possible that the car actually brings certain kinds of equipment with them to use in the field as well (portable ultrasounds, equipment for blood draws, etc) and it becomes a mobile clinic.
- Will society have the…chill required to handle public sleeper cars. I’ve seen what people do on the subway so my answer is no.
Mobile pharmacies - In the same way you have pharmacy vending machines and courier delivery pharmacies like Capsule, autonomous cars could pave the way for mobile vending pharmacies. The prescription is sent to a central pharmacy, and then an autonomous car is loaded up with all the orders which you go out and grab after it checks your identity.
Door-to-door sample collection - If you need to take a sample collection of anything at home, it’s really annoying to bring it to UPS or wherever it’s supposed to go. One way to really lower friction is a car outfitted with temperature control, vibration proof storage, and anything else needed to verify chain of custody. I want a shit chauffeur for my colon cancer screening.
Hospital Parking Revenue Goes Down
If the main method of transport becomes driverless cars, you won’t actually need to park your car at the hospital.
A lot of patients and employees pay for parking at hospitals. Operating a parking lot isn’t free and many other countries also charge for their parking lots (e.g. the NHS has an entire wikipedia page dedicated to it because paying for anything related to healthcare in the UK is a controversy).
For hospitals it’s usually a very small portion of revenue - Cedars-Sinai for example made more than $14M from parking revenues but it's a tiny fraction of their $4.6B total revenue.
But there are some scenarios where a developer or real estate company owns a chunk of land and parking is a bigger part of their revenue. Texas Medical Center is probably the most extreme examples of this - Bob Herman from STAT News wrote this:
“The Texas Medical Center is essentially a manager that watches over Houston’s sprawling complex of academic hospitals. It operates more than two dozen parking garages and lots. If you’re there for an hour or less, it’ll cost you $5. An overnight stay will cost you $19. A lost ticket will set you back $30.
TMC generated $81 million from parking fees last year, making up more than half of the organization’s annual revenue. The average visitor paid about $33 for parking, based on TMC’s 2.48 million parking visitors last year. Another $33 million of revenue was classified as investment income. In other words, TMC is a hedge fund that is financed by everyone’s parking fees.” - STAT News
These operators will probably see more of their revenue at risk, which could mean charging the companies on their campus more money or providing more value-add services.
This then raises the question of what’ll be done with some of these parking lots near hospitals if demand shrinks? More likely than not, they’ll just expand their facilities, duh.
Older People will be More Willing to Age at Home
This one isn’t really grounded in much data but more vibes. Actually nvm, this entire thing is vibes.
I’m at the age now where a bunch of my friends have aging parents. It’s the natural cycle of life, except for me since I’m shooting NAD+ straight into my gonads because the longevity guy said I should.
One big argument for parents to get rid of the car and stop driving is because their vision is getting worse or their health is failing. But for most parents, the car is basically their only means of staying independent - which starts a conversation about moving into a nursing home.
I wonder if the ability to summon self-driving cars delays older people from moving into some form of nursing home, and you’ll see more people aging in place for longer. Now again, any serious health issue will still probably require them to stay in a place that has oversight/aides independent of driving.
But the ability to move around or get things delivered for cheaper might make it easier for older people to live independently.

Environmental Health Benefits
A predominant belief is that self-driving cars will boost electric vehicles. Most autonomous cars are electric because electric vehicles are way simpler to operate, cheaper for fleets, and the onboard computing needed to be autonomous requires a lot of electricity. Waymos are all electric, Tesla is electric, and all the Chinese self-driving cars are electric.
So a second order effect of self driving will be electric vehicles becoming the predominant car on the road. What are the THIRD order consequences of what that means for healthcare?
There’s quite a bit of literature now that combustion engine output causes worse health outcomes for people exposed to them regularly. One of my favorite studies looked at EZ-pass being rolled out. Cars went through faster so there was less congestion, which meant less emissions around the toll areas. After the roll out there was a pretty significant drop in premature/low weight births for people near the toll areas. More recently, a study looked at zip codes in California and found that as electric vehicles increased, asthma-related emergency department visits dropped 3.2%.

I do think near highways and freeways, you’ll see less noise and emission pollution. This should yield some population health benefits, right before property values go up in that area and they get pushed out.
Featured Jobs
Some people are hiring!
Medicircle - Operations Director (New York or Sugar Land / Houston Metro Area)
- MediCircle lowers drug costs for patients and health plans by reclaiming and recertifying unused medications. This hire will partner with our COO to systematize and optimize the operational workflows that enable efficient and compliant medication donation and redistribution at scale. Apply here.
Greenbrook Medical - Chief of Staff (New York City, NY)
- Come join Greenbrook Medical, an at-risk primary care group serving MA members, as our Chief of Staff. You’ll work closely with our leadership team to execute strategic priorities and scale a strong foundation into something extraordinary. Perfect role for an aspiring leader. Apply here.
Turquoise Health - Group PM, Contracting Product (Remote, US)
- Lead AI- and ML-driven products that reshape back-office healthcare and reimbursement processes, replacing legacy contracting systems with smarter workflows. Success means using AI with creativity and sound judgment to transform healthcare contracting, helping us operate at a higher level. Apply here.
Meta Level - the Autonomous Car vs. Doc Parallels
I think that the way society views autonomous cars will probably be similar to AI doctors. It's a complex task, requires a level of specialized skill and license to do it, and the downside risks if it’s wrong are enormous. Yet after many years autonomous cars are on the road, expanding quickly, and creating new awkward social scenarios.
Autonomy in cars has been measured in five levels, depending on how much the human needs to be involved. The California Public Utilities Commission has a formal program to test capabilities (e.g. specific geographies, times of day, weather, human oversight, etc.). The DMV also requires crash reporting and data the public could see.
Healthcare probably needs to adopt a similarly common grading scale of autonomy and clear pathways to test AI with human oversight. Sebastian Caliri from 8VC drew up a version with four levels that could work well, with each level having a different level of evaluation, ability, and billing. The new Doctronic pilot in Utah for an AI that can prescribe starts with a lower risk and contain task - medication renewal for 190 drugs with human oversight and auditability.

I’m glad autonomous cars laid the groundwork for what a high stakes AI rollout would actually look like. Healthcare seems to be following a similar rollout, and I hope it won’t take eight years like it has with autonomous vehicles. I’d be able to go back to med school and be the last person to get their medical license too.
Conclusion and Parting Thoughts
A colleague of mine took a lap in a self-driving car in 2015 at CES. I really thought it wouldn’t be until I was 50+ for this to be on the road. And yet it’s so normal now that whenever I come to SF I’m not even phased when one pulls up.
I remember being in one as an inflection point for my optimism about the future of technology. I hope we have more of that.
Thinkboi out,
Nikhil aka. “All drive no driver” aka. “move Fast and break things Furiously”
Twitter: @nikillinit
IG: @outofpockethealth
Other posts: outofpocket.health/posts
{{sub-form}}
If you’re enjoying the newsletter, do me a solid and shoot this over to a friend or healthcare slack channel and tell them to sign up. The line between unemployment and founder of a startup is traction and whether your parents believe you have a job.
Interlude - Apply to Knowledgefest! And healthcare 101 starts next week!
See All Courses →Don’t forget the application for our Knowledgefest, our healthcare software engineering conference IS LIVE.
If you work in healthcare ops, you want to be here. This is where you learn playbooks, see what other ops people are doing, and build your network. It’s year 5 and we sell out every year - applications are due end of month.
And if you feel like you really need to get up to speed on how healthcare works, then you should let me teach you at Healthcare 101starting next week!This is for anyone hiring teams of non-healthcare people that need to get up to speed quickly (in 2 weeks) - we do group discounts too hit up ya boy. You’ll even learn how to make memes.
.png)
Get Out-Of-Pocket in your email


