




The debate around pharma advertising to doctors (part 2)
Get Out-Of-Pocket in your email
Looking to hire the best talent in healthcare? Check out the OOP Talent Collective - where vetted candidates are looking for their next gig. Learn more here or check it out yourself.
 Hire from the Out-Of-Pocket talent collective
Hire from the Out-Of-Pocket talent collectiveHealthcare 101 Crash Course
%2520(1).gif)
Featured Jobs
Finance Associate - Spark Advisors
- Spark Advisors helps seniors enroll in Medicare and understand their benefits by monitoring coverage, figuring out the right benefits, and deal with insurance issues. They're hiring a finance associate.
- firsthand is building technology and services to dramatically change the lives of those with serious mental illness who have fallen through the gaps in the safety net. They are hiring a data engineer to build first of its kind infrastructure to empower their peer-led care team.
- J2 Health brings together best in class data and purpose built software to enable healthcare organizations to optimize provider network performance. They're hiring a data scientist.
Looking for a job in health tech? Check out the other awesome healthcare jobs on the job board + give your preferences to get alerted to new postings.
This episode of Out-Of-Pocket is brought to you by…
Over the last decade, Ursa Health has quietly powered some of the most innovative names in value-based care.
See how Cityblock Health ditched black box analytics and built a transparent, adaptable quality engine that seamlessly integrates EHR, claims, and clinical data. By combining flexible logic and near real-time data, insights don’t just sit in a dashboard- they drive action.
If you're thinking seriously about VBC data infrastructure at scale, this case study is worth your time.
—
We got our content schedule for the next few months. Let’s chat sponsorship, maybe there’s a topic that’s relevant to your company.
Does Nikhil have a point or should we clap back?
Last time I talked about how I think advertising-based models to doctors are fine, specifically in the light of OpenEvidence/DoxGPT.
I asked you all what you thought and got some GREAT responses. I was actually encouraged that people live along various points of the spectrum on this topic, debate is good.
You can see some curated responses below. Memes and commentary added by me.
Showing prices does work!
“Generally I’m with you. People are skimming our decision making all day long and probably monetizing that data anyway (cough cough Epic). You could offer people an opt out where they pay for Open Evidence instead of it being free and then it’s ad and conflict free for them. I don’t think you’d have many takers.
As an aside- I love the idea of hitting the doc with the drug price at the time of the encounter. We did a pilot project in the OR one year in residency where the nurse called out the price of the equipment/disposable that the surgeon asked for. Utilization rates plummeted. You just have to make it transparent.”
Josip Vukuna
[NK note: Honestly I think 80% of sins in US healthcare could be solved by just showing prices for things. And I’m tired of pretending that’s not the case.]
{{interlude 3}}
Ads will erode the patient<>doctor trust
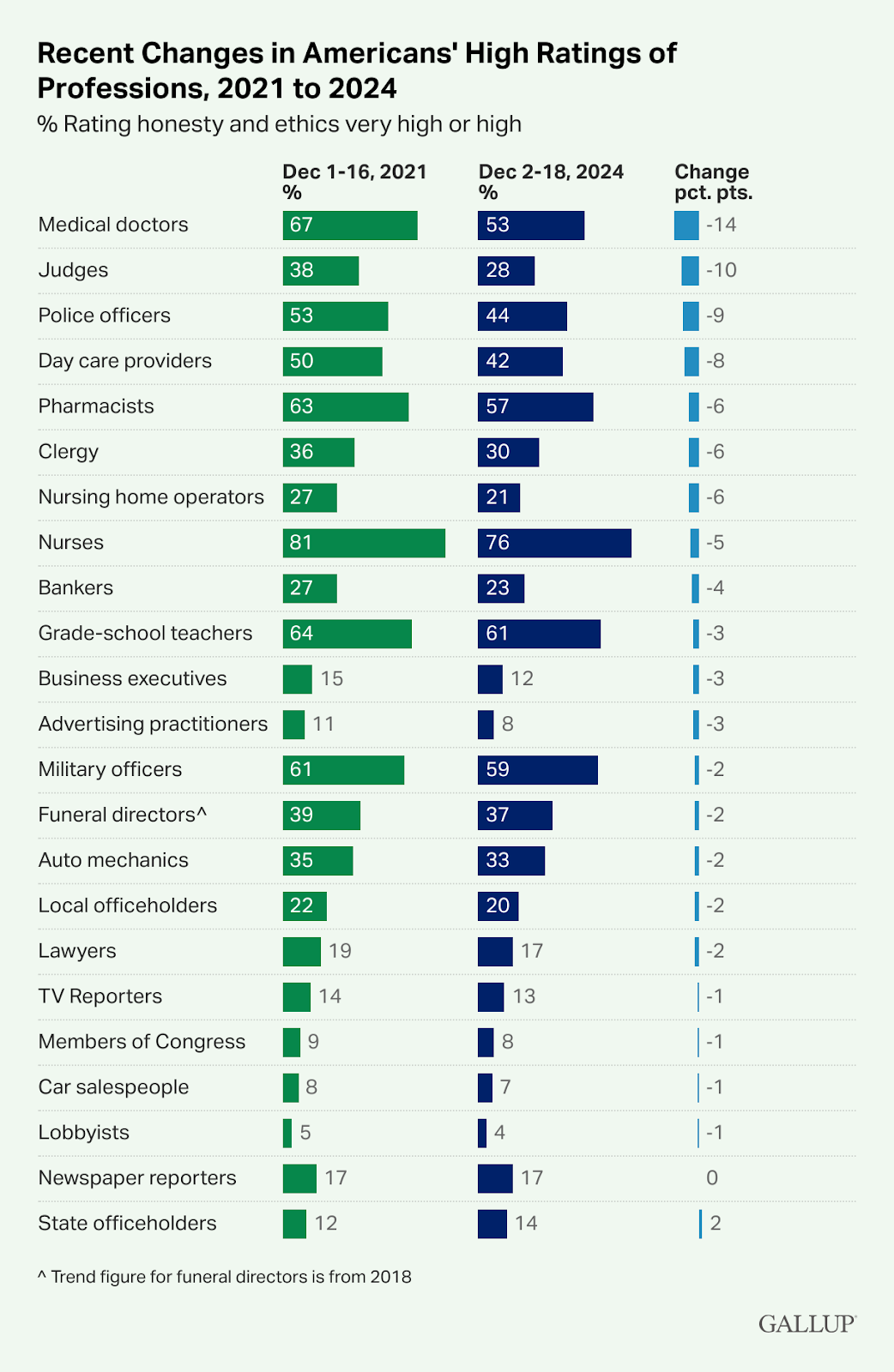
“While I agree that ads can be useful for clinicians by improving visibility of available drugs and the evidence behind them, the risk is that it further erodes doctor-patient trust, independent of whether the treatment is actually better in the counterfactual and whether the recommendation is in good faith. Trust is already trending down (Gallup data shows a 14-point drop since 2021, the largest of any profession measured), and movements like MAHA are making it fashionable to question your GP. If patients got whiff of advertising embedded in the clinical tools guiding their care, there's a chance that a meaningful chunk of the patient population will begin to question their clinician's judgement and seek alternative answers, delaying care and causing more harm and $$$ down the track.
Funny thing is that clinicians are already flooded with pharma advertising through other channels, which I think patients accept, but for whatever reason, once you add AI into the mix, people lose their minds and question everything. Ultimately it comes back to the trade-off between value and risk. In primary care settings, where the doctor-patient relationship is ongoing and trust is the foundation, ads are likely a net negative. In specialist and tertiary settings, particularly where patients face more acute needs and clinicians are making narrower, evidence-driven decisions, the case for them is stronger.”
[NK note: I agree with this largely. But can someone tell me what…would increase trust in doctors at this point? It seems like anything docs do now lowers trust with the public. A doc could save a baby from a burning building and there would be a viral tweet about how the doc probably started the fire.
But I’m sympathetic to this point, I do think this in particular might make patients feel uneasy if they saw it.]
There’s a new principal agent problem
“What’s missing from your argument on ads in digital products is that it introduces a new user (the buyer) with new incentives that takes away attention (at best) or degrades (at worst) from building an awesome product for doctors (or whomever the primary user is).
Growing ad revenue usually relies on more surface area or more targeting. Open Evidence has said publicly that they don’t slow down results returning to show ads (more surface area), but the fact that they even mention it tells me that it’s entered the conversation.
There’s a long history of products degrading because of ad models, it would be a shame to see the same happen to such a beneficial product, particularly when there’s precedent for paying for access. At minimum, I hope that the targeting and product changes are made transparent for doctors so they know how their experience is being influenced by getting something for free.”
[NK response: totally fair - I will say that it's the tradeoffs vs selling through enterprises, which are also a different buyer than users. It's why all the tools doctors use at hospitals are terrible. Or Stevie Wonder is their head of design.
Either way you're dealing with some principal agent problem, but at least if it's ads then there's some ad load presumably where a user would switch if it gets too bad. There aren't REALLY network effects for these tools (yet) so they don't have as strong lock in. Look how much all of these scribe/literature review/clinical decision support companies have to compete with each other by adding new features and integrations. Now look at how much the other provider software has improved in that same time period. Competition feels net good for users!]
Let the market cook
“Classic healthcare, taking an issue we're wrestling with in a general sense, and make it even more complicated.
We've all made the devil's bargain of offering up our data in exchange for awesome free stuff (imagine if I tried to stop using Google products?). So I'm on board with this model finding its way into physician workflows. As you noted, healthcare is still super paywalled and it sucks. But not only for individuals; at a systems level, it's yet another force pushing toward consolidation because only the big health systems can afford all these expensive enterprise resources.
Do ads influence physician behaviors? I think it's pretty clear that they do, and some older research corroborates that. Maybe the answer then is to let the market do its work -- what if there were incentives for payers, health systems, and even professional societies to take out their own ads? Not sure exactly what that would look like, or if physicians would feel comfortable being caught in the middle of an influence campaign (aren't they already though?), but it beats pretending we're all okay with the status quo. As a litmus test, shut down OpenEvidence and all its competitors for a week, then poll physicians on whether they'd accept advertising in exchange for getting access restored.”
[NK note: Ads are a sign of an actually competitive market - it means that companies need to actually TRY to get customers. In a certain light, the lack of advertising in healthcare is sort of reflective that no one really has to compete. Maybe we need more ads??? Which podcaster is brave enough to get sponsored by a PBM??]
We’re already in an ad shaped world
“Fundamentally, I don't think it matters if you're advertising to docs on these platforms or not. First of all, this is literally the business model for every major tech company. Even if you think it's wrong, it's going to continue happening. Opportunity to advertise and data are two of the biggest commodities in today's economy. We can argue about the placement of these ads (i.e when a physician is presumably performing some level of patient care and is being targeted almost at the point of the encounter), but I don't actually think it will matter that much.
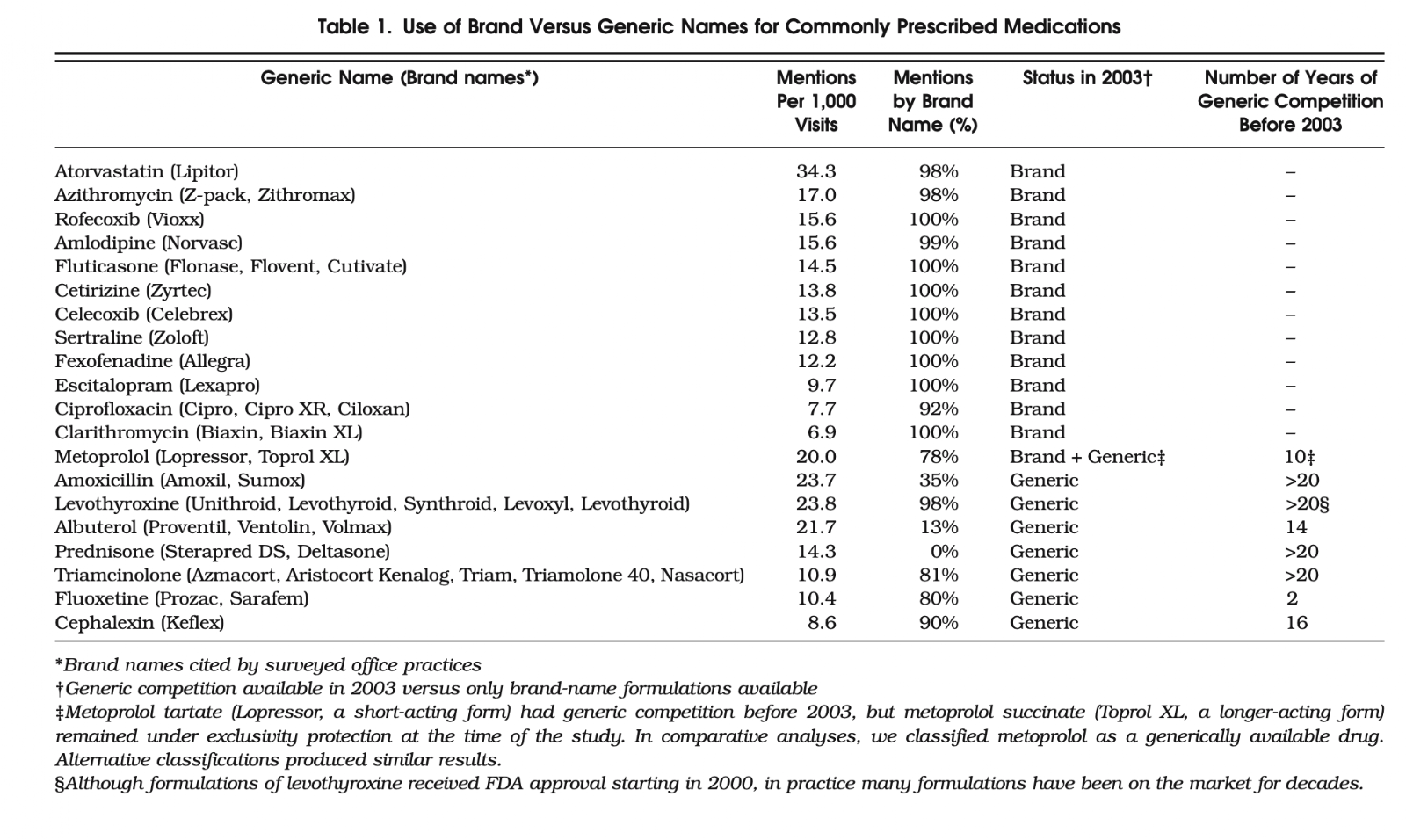
Let's think about pharma here, where I would see the most obvious conflict of interest. There's already pretty good data that shows physicians predominantly use brand names instead of generic names for drugs, even if there are generic formulations available. One study cited this at 98% for the top 20 medications prescribed. This was a bit of an older study (2007), but the point is that physicians have been influenced by the pharmaceutical industry en masse to the point where the medication is not even referred to by the clinical name, rather the brand name.
Regardless of how prescribing habits are impacted, the advertisement of these drugs has already reached peak performance. Seeing a tremfya commercial while researching about Crohn's disease is kind of a moot point. That also assumes that the ads become very specifically targeted.
And from a cost perspective, it's something like 70% of the drug expenditures in the US come from ~10% of all drugs. Obviously there is asymmetry due to patent timelines, but I suspect a large part of this is also just driven by the sales and marketing tactics that the pharmaceutical companies have already employed. They're gonna keep advertising as much as possible because it has been quite effective thus far. If they do it on a platform that allows physicians to access knowledge/literature more easily and possibly take better care of their patients, who cares? I don't think it will actually make that much of a difference in driving more conflicts of interest.
BTW I used open evidence to search for some of the data while writing this. I entered my query, left before seeing an ad, and then returned when the response was ready. So maybe all these ads will have very low conversion? Hah”
[NK note: The other practical question here is…how would you even police this? Okay you can’t advertise for literature review, can you literally put a TV in a doctor's office and run ads on the TV? Could you take out billboards near hospitals and clinics? I’m just not even totally sure how you would prevent ads from influencing docs.]

Pharma ads are the easiest spend
“Sharing a few thoughts from the pharma perspective. I know this isn't the question you're asking but if you want money from pharma, I think advertising might be the only scalable way to do it.
I think this is a much lower compliance risk for pharma, relative to paying for a solution/access to a solution for doctors. I assume it would be a similar approval process to a TV ad (where you take little/no responsibility for what else is shown on the TV channel before or after your ad).
Compared with paying for a solution, where you need to review everything. For a pharma app we worked on, all screens had to be reviewed in pdf including the generic apple/android pop-up screen that says "turn on bluetooth". In Android and iOS. 1000+ screenshots.
Reviewing all text is also a big challenge for pharma to use AI solutions. I think some pharma companies have found solutions but may be dependent on risk appetite.
So advertising may be the best option to get pharma to pay for something AI-based. And you could assume pharma advertising budgets are 10% of revenue which is a lot bigger than the "let's do something with AI" budget.”
- Anonymous
[NK note: Everyone wants a bag from pharma, but it’s important to figure out:
- Which budgets it’s coming from
- How easy is it to deploy from an existing budget
- How much work is it to get the money
As someone who has tried to get marketing dollars from larger companies, what I’ve learned is the more “new” something looks, the harder it is to get approved internally, and the less likely you’re gonna get the bag. So if you can sell something within their existing processes you’re gonna have a much easier time.
Selling apps to Pharma was the rage in 2018, now I understand why that didn’t work out as well.]
Ads to patients are eroding trust
I think the logic is much more simple. New expensive medications enter the market based on evidence. They need marketing push to get out there. If they're successful and have evidence, they will get traction. If they aren't they won't. This is correlation, not causation.
I don't eat lunch so I don't have to talk to reps when in clinic. I also pay for Disney+ cause my kids don't have patience for ads. The only people who got the pharma pens were the people who let the reps in in the first place. Relationships drive every B2B sale in every industry. But nobody is dragging admin in for taking a demo over lunch from Epic.
That being said, when I hear a patient tell me that Jardiance is the medication with "that catchy song" and that's why they don't want to take it, despite overwhelming evidence that it 1. reduces mortality. 2. helps with diabetes. 3. helps with CAD. 4. Helps with HF. 5. Helps with CKD.

Then I literally have to tell the patients that - ‘if it wasn't effective and profitable, they wouldn't advertise for it on tv.’ or ‘you know those lawyers out there talking about eliquis in their ads? They wouldn't be doing that if it wasn't an important medication.’
48% of physicians in one study admitted they prescribed a DTC-advertised drug they clinically disagreed with just to keep the patient happy. The advertising isn't influencing doctors. It's influencing patients, and then institutions punish doctors for saying no.
So actually, in retrospect, advertising actually makes my job of delivering effective medical therapy harder in every way.”
-Anonymous Doc
[NK note: This was interesting - it’s another example of where I think we expect doctors to absorb everyone else’s sins and allow them to do no wrong. We put them under a microscope if pharma reimbursed then $16 for a sandwich but don’t do the same with other parts of the healthcare apparatus that then affects how docs practice (e.g. hospital admin choosing tools they have to use).
I also do wonder how true the “if they have evidence, they will get traction” thing is. I haven’t looked deeply at this, but I could also see a world in which companies with pretty “eh” results spend a lot on marketing because they know the evidence won’t speak for itself. There’s tons of approved drugs out there with pretty questionable data on how well they actually work for outcomes that matter]
Featured Jobs
A few companies are hiring! Tell em OOP sent you.
Parakeet Health - Customer Success Manager (SF, In-Person)
- Healthcare still runs on hold music and fax machines. Our AI agents handle calls, faxes, and patient outreach for practices across all 50 states -- automating the most tedious admin tasks. We're hiring CSM #2 to help practices transition to this agentic world. Lean, ambitious, and AI-pilled team. Apply Here.
Blueberry Pediatrics - Senior or Staff Full-Stack Software Engineer (Remote)
- Healthcare is seldom affordable, accessible, or high-quality. We’re fixing this for pediatrics. Blueberry is the most affordable VBC option on the market, available 24/7, driven by MDs. We’re looking for senior or staff-level full-stack product engineers to advance our mission. Apply here.
Photon - Head of Platform Partnerships (Brooklyn, NY)
- Photon is a prescription marketplace that helps millions of patients compare pharmacies by price and convenience. We're looking for someone to own EHR and platform partnerships with a focus on driving Rx volume. Ground-floor role reporting directly to the CEO. Apply here.
Do ads incentivize the wrong things?
When business models reward clicks and impressions over evidence-based care, commercial priorities override clinical ones. OpenEvidence is used by 760,000 US doctors and charges pharma companies to place ads at the point of care, right when a doctor is searching for treatment guidance.
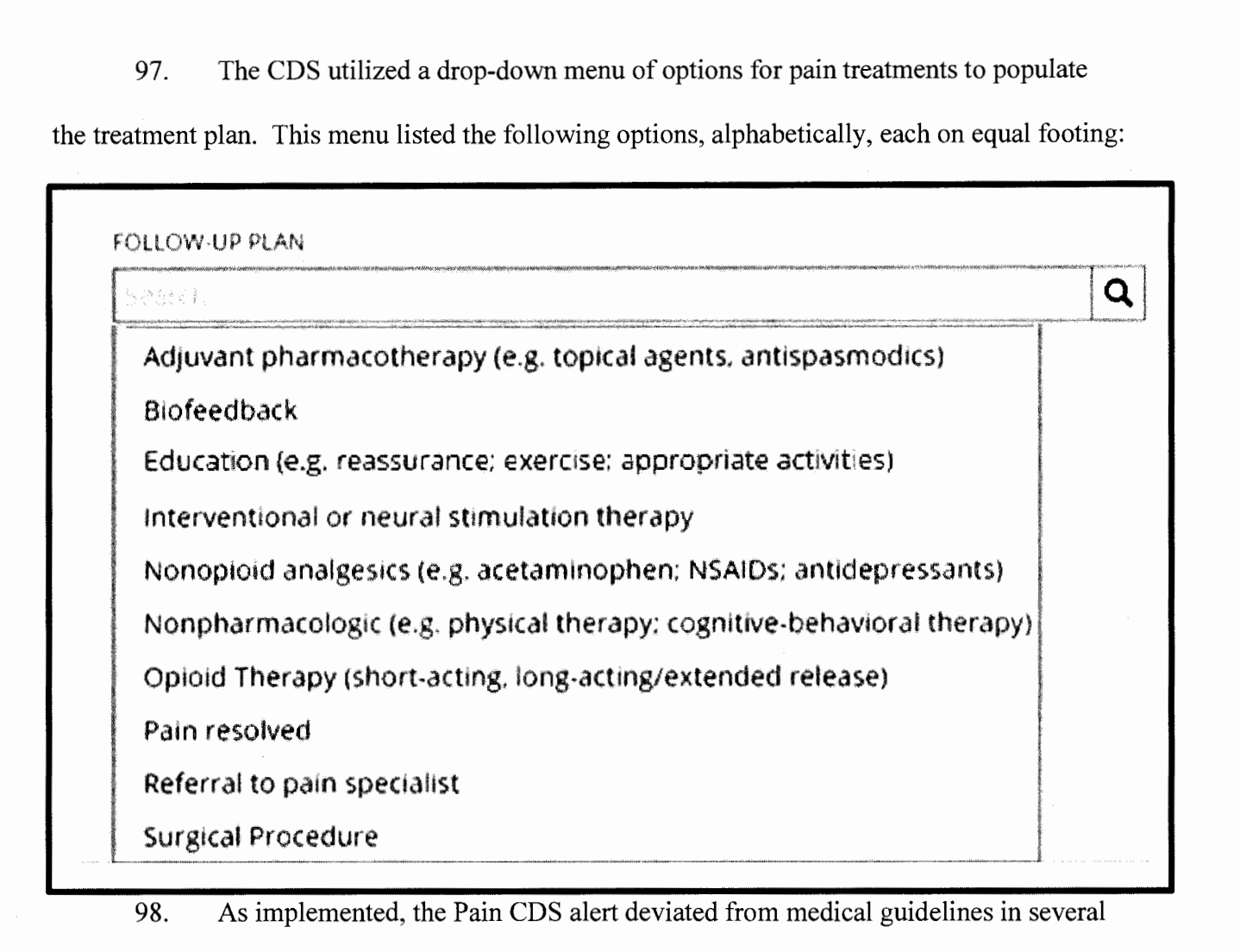
We've seen how this ends. Practice Fusion was paid to embed clinical alerts that steered doctors toward opioid prescriptions. Those alerts were triggered 230 million times before anyone was held accountable. And while the company was fined $145M, you can't undo 230 million clinical decisions.
AI will only continue to make this worse as engagement patterns feed back into model training over time. We won't just repeat the mistakes of the past. We could automate them at a scale that would make the opioid crisis look small.
Free and ethical aren't mutually exclusive. But it requires a business model that serves clinicians, not advertisers. If your doctor's decisions were sponsored by pharma, would you still trust them? I think it's time for a second opinion.
[NK note: I think there are very valid concerns around tools that can cause impact at scale like this, and I do think there has to be some watchdogging or audits of some kind to watch out for that. This is why I said that form factor matters in the last post - Practice Fusion was particularly bad because it looks like it’s part of the regular workflow.
But it’s not exactly clear to me that this is unique to a pharma advertising model? For example Epic got a lot of flak for the issues in their sepsis detection AI which is also a clinical decision support tool at scale and not an ad-based model.
I can’t pretend like I wouldn’t be a little sussed out if a doc wore a pharma logo on their whitecoat for example. But also I probably SHOULD be a bit more skeptical of how the hospital they work out also influences the downstream decision making. The reality is that doctors are humans just like any of us and are influenced by lots of different things - eventually you just have to put some trust in them that they’re making the best call for you taking those influences into account.]
Conclusion and parting thoughts
This was fun, I may have slightly changed my mind around this topic thanks to your responses. Appreciate everyone who phoned in.
If you have any good discussion questions I should ask this newsletter in the future, let me know. I think we get some great responses.
Thinkboi out,
Nikhil aka. “Betting the pharm” aka. “Damn anyone suddenly have the urge to get an ice cold Rinvoq?”
Twitter: @nikillinit
IG: @outofpockethealth
Other posts: outofpocket.health/posts
If you’re enjoying the newsletter, do me a solid and shoot this over to a friend or healthcare slack channel and tell them to sign up. The line between unemployment and founder of a startup is traction and whether your parents believe you have a job.
Interlude - Apply to Ship It! And Healthcare 101!
See All Courses →Don’t forget the application for our SHIP IT, our healthcare software engineering conference IS LIVE.
If you write or deeply work with code, have some experience working in healthcare, and want to has out how everyone is building things…you should apply to this. It’s small, intimate, and you’ll learn a lot.

And if you feel like you really need to get up to speed on how healthcare works, then you should let me teach you at Healthcare 101 starting 7/13!
This is for anyone hiring teams of non-healthcare people that need to get up to speed quickly (in 2 weeks) - we do group discounts too hit up ya boy. You’ll even learn how to make memes.

Get Out-Of-Pocket in your email


