




Advertising to doctors - okay or not?
Get Out-Of-Pocket in your email
Looking to hire the best talent in healthcare? Check out the OOP Talent Collective - where vetted candidates are looking for their next gig. Learn more here or check it out yourself.
 Hire from the Out-Of-Pocket talent collective
Hire from the Out-Of-Pocket talent collectiveFHIR 101

Featured Jobs
Finance Associate - Spark Advisors
- Spark Advisors helps seniors enroll in Medicare and understand their benefits by monitoring coverage, figuring out the right benefits, and deal with insurance issues. They're hiring a finance associate.
- firsthand is building technology and services to dramatically change the lives of those with serious mental illness who have fallen through the gaps in the safety net. They are hiring a data engineer to build first of its kind infrastructure to empower their peer-led care team.
- J2 Health brings together best in class data and purpose built software to enable healthcare organizations to optimize provider network performance. They're hiring a data scientist.
Looking for a job in health tech? Check out the other awesome healthcare jobs on the job board + give your preferences to get alerted to new postings.
Ads aren’t that bad, let’s fight
OpenEvidence, DoxGPT, and a few other tools are vying to be the ChatGPT for doctors by using AI for literature review. It’s incredible to hear doctors talk about a tool they like using, I can’t wait to show them how to use Google Calendar next.
These tools are free for any doctor with an NPI number to use a HIPAA compliant version. Companies pay to run ads (video, banners, sponsored content) while physicians use the platform. The bulk of ads seem to be for research, literature, and courses. But I’ve also started seeing pharma ads slowly making their way in, which is a logical next step.
I wrote a longer post about the opportunity for direct-to-employee tools and how advertising is an enabling model, but I got a lot of interesting replies to that. So I figured I’d make it into today's discussion post.
What do you think about advertising to physicians and monetizing their data as a business model? I’ll use pharma advertising and data mining as the core use case here.
A few random thoughts. I don’t feel strong in these opinions and might change my mind tomorrow.

1. Free is more accessible
UpToDate costs $550+/year per physician. OpenEvidence being free means any physician can access AI-assisted evidence lookup regardless of where they practice or how much their employer spends on IT. I think it’s bad to keep stacking fees on top of doctors/providers - you can think of this as a way to shift those expenses to pharma instead.
My belief is that getting AI tools in the hands of doctors as a clinical decision assist is important and a net benefit for society. So we should try to reduce the barriers to doing that. If using an advertising based model speeds that up, then that’s probably net good.
This also puts competitive pressure on the legacy providers who've been charging $550+/seat for decades. UpToDate now has to justify its price against a free alternative that physicians are voluntarily choosing. That kind of market pressure is healthy and means UpToDate has to provide $550 of value that feels worthwhile.
{{interlude 3}}
Back to our programming.
2. The form factor of the advertising matters a lot
I do think HOW an ad gets presented is important. For example, PracticeFusion is the best example of how to not do this. They were an EHR that was free to doctors funded by advertising. In 2020, the DOJ hit them with a $145 million settlement because an opioid manufacturer paid them to design clinical decision support alerts inside the EHR. If a patient reported pain of 4+ on a pain scale twice within four months, the system would pop up a care plan that included "Opioid Therapy" as a treatment option. But this wasn't labeled as sponsored, the doctor would just think this is a decision support tool.
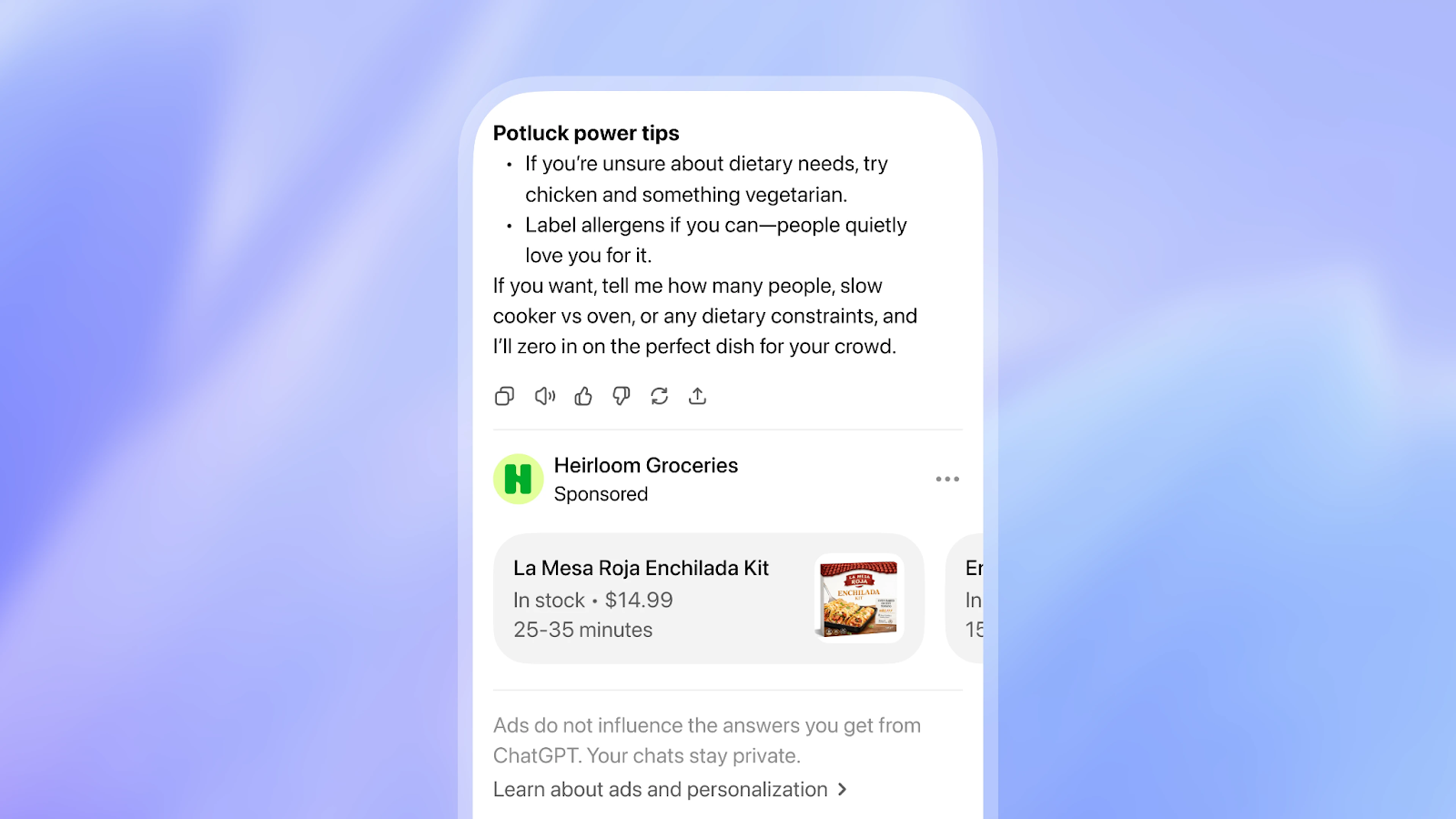
Based on what I’ve seen, when you use OpenEvidence they’ll show you an ad while the AI is reasoning and building your answer. It’s pretty clear that it’s an ad, and then your answers are presented after. When the ad is clear to the user, I think it’s less of an issue.
But this can get murky! For example what if the literature summarized includes industry funded studies without flagging who paid for it? When doctors read literature themselves do they look out for that all the time and factor that into their decision making? I do think we might need flags around the sources and whether they’re industry funded.
3. De-identified data going to pharma is probably fine?
What if OpenEvidence/DoxGPT collect information about what doctors are searching for and sell that de-identified to pharma companies? Pharma is going to find out I *checks note* feel some weird new sensation in a different joint and it turns out that’s called “regular aging”.
Honestly, I don't think selling de-identified data is that bad? Pharma is already stitching together a pretty detailed picture of physician prescribing behavior from pharmacy claims data, EHR data, medical claims, etc. It’s not entirely clear that this is that different - this would probably just take revenue from other data sources that pharma normally pays for.
Maybe having a more accurate account for why doctors and patients are switching drugs might help the R&D pipeline, but maybe that’s me being too optimistic about how this data would be used.
4. Are highly relevant ads good or bad?
Most pharma ads are general brand awareness of a drug. This is one of the reasons the ads feel so jarring - they’re typically irrelevant to the context they’re presented in.
If doctors start doing literature review at the point of care with context about the patient and a highly relevant drug or industry-funded research is served, is that good or bad? It might actually be more useful for the patient, but also means the doc is more likely to be fr influenced.
It’s kind of like comparing instagram ads (highly relevant and actually serving things I’d probably buy) vs. Twitter ads (embarrassing to see, borderline gooner content).
I go back and forth on this, but I tend to lean that having highly relevant ads that can ACTUALLY help with discovery of new products and papers is a good thing. But I can see both sides here.

5. The problems people put on advertising are actually problems of cost-effectiveness
IMO the big issue is not that physicians are influenced, but rather that cost is not one of the factors that influence them. When a doc is choosing an IL-23 inhibitor that seems to have similar efficacy for the given patient or they just need to try any of them for a first line treatment, why not try the one that has the most fun jingle? The reason is because each of them costs very different amounts and have different coverage per insurance, but that typically isn’t in the calculus for the doc or the patient especially if the insurance is the one paying for the bulk of it.

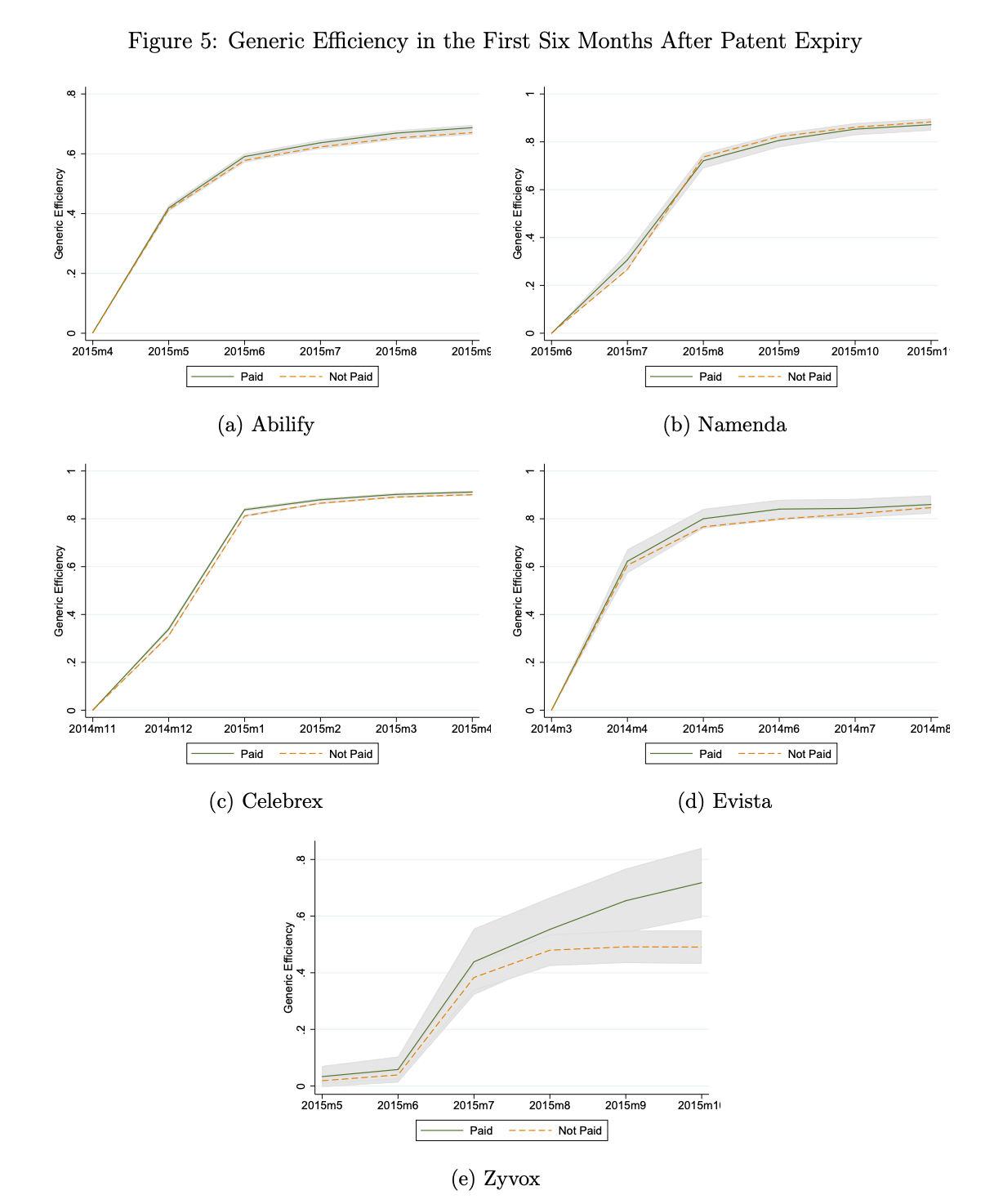
If there was more transparency around how much the drug would end up costing (either insurance or patients), then maybe the advertising would matter less? As an example, even when doctors are paid by a pharma company they still switch patients to generics when they become available. There is an understanding that the generic drugs will be cheaper, more accessible, and about the same as the branded drug even if the physician is “influenced” by the pharma company.
Maybe making that cost-effectiveness clear at the point of decision making between drugs might have a stronger influence on decisions than the ads.
A few featured healthcare jobs
Some cool companies are hiring!
Parakeet Health - Customer Success Manager (SF, In-Person)
- Healthcare still runs on hold music and fax machines. Our AI agents handle calls, faxes, and patient outreach for practices across all 50 states -- automating the most tedious admin tasks. We're hiring CSM #2 to help practices transition to this agentic world. Lean, ambitious, and AI-pilled team. Apply Here.
Omada Health - Senior Analyst, Strategic Finance (Remote working EST)
- Partner with leaders to structure complex deals, analyze engagement trends, build revenue forecasts, and turn large data sets into insights. Requires 3+ years in Finance, Consulting, or BizOps, strong modeling, SQL, and communication skills. Apply here.
Daymark health - Product Manager (East Coast)
- Cancer care is broken and Daymark Health is fixing it. Join a team that's building technology that supports patients and care teams through one of life's hardest experiences. Apply here!
Where I land (for now)
I think the free + ad-supported model is net positive for physician access. I think the form factor concerns are real but manageable if the company maintains genuine separation between ads and clinical content. This might require independent audits that the ads are not influencing the literature review itself.
At a high-level, I’m pro advertising. Out-Of-Pocket is ad funded, and that’s because I think it’s important for content to be accessible to people and the ideas be distributed. Getting information into the hands of people is the most important thing we can do IMO vs. put it behind paywalls (don’t quote this when I sell out and go behind a paywall though).
Vilifying ad funded products is understandable, but they present a different set of tradeoffs just like paid products do. The core question: Is making AI tools really easy to access a net positive relative to the amount of influence the ads actually have? And is it possible to have the ads actually yield “not that bad” influencing?
Idk, I go back and forth. But I don’t think it’s AS bad as everyone says. Crucify me, I’m ready.
What do you think about advertising to physicians and monetizing their data as a business model? I’ll put my favorite responses in the next newsletter.
Thinkboi out,
Nikhil aka. “Pushin P(harma products)” aka. “Ask your doctor if ads are right for you”
Twitter: @nikillinit
IG: @outofpockethealth
Other posts: outofpocket.health/posts
If you’re enjoying the newsletter, do me a solid and shoot this over to a friend or healthcare slack channel and tell them to sign up. The line between unemployment and founder of a startup is traction and whether your parents believe you have a job.
Quick Interlude - NEW COURSE ON FHIR! KNOWLEDGEFEST APPS DUE SOON!
See All Courses →So...what actually is FHIR? I get this question a lot, but there's never really enough time to explain it and also I would just mumble "technical standard" and walk away.
So we decided to do a standalone free FHIR 101 course in partnership with Redox! Over 3 days in August we'll go over the spec itself, how it differs from other healthcare information standards, and practical tips to build with it.
I wanted to call it FHIR fest but it got nixed. You can sign up for it here, it's FREE and it's 8/25-8/27.

And a reminder that Knowledgefest apps are due this week. If you want to be in a room with the best ops people in healthcare, you should apply like TODAY.
We sell this conference out every year - all workshops, learn how people are building and scaling in healthcare, application based so we only take the best. We have people from Commure, Clarity Pediatrics, Pomelo, and Waymark already coming, join the squad.

Get Out-Of-Pocket in your email


