




OpenEvidence and the Opportunity In Direct-To-Employee Tools
Get Out-Of-Pocket in your email
Looking to hire the best talent in healthcare? Check out the OOP Talent Collective - where vetted candidates are looking for their next gig. Learn more here or check it out yourself.
 Hire from the Out-Of-Pocket talent collective
Hire from the Out-Of-Pocket talent collectiveHealthcare 101 Crash Course
%2520(1).gif)
Featured Jobs
Finance Associate - Spark Advisors
- Spark Advisors helps seniors enroll in Medicare and understand their benefits by monitoring coverage, figuring out the right benefits, and deal with insurance issues. They're hiring a finance associate.
- firsthand is building technology and services to dramatically change the lives of those with serious mental illness who have fallen through the gaps in the safety net. They are hiring a data engineer to build first of its kind infrastructure to empower their peer-led care team.
- J2 Health brings together best in class data and purpose built software to enable healthcare organizations to optimize provider network performance. They're hiring a data scientist.
Looking for a job in health tech? Check out the other awesome healthcare jobs on the job board + give your preferences to get alerted to new postings.
It’s time to build tools directly for healthcare employees
When I do my healthcare 101 course (next round starts 12/1!!!), in the first lesson we talk about how healthcare is rife with the principal-agent problem. The entities who pay for things and the entities that use products/services are usually two different people.
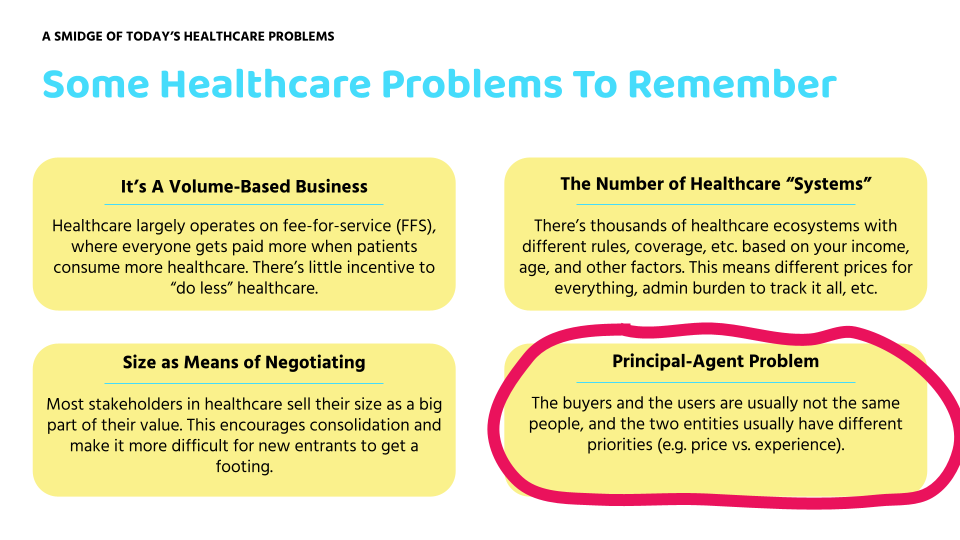
As healthcare continues to consolidate, one place in particular you see this show up is that the tools that frontline workers have to use are paid for and chosen by a procurement/administrative layer. This means that the main considerations are price and the breadth of features included in it. The actual user experience is lower priority.
However I believe we’re now seeing new opportunities to build tools catered to employees and frontline workers. This is for a few reasons.
- Tons of healthcare workers that absolutely hate the software that they use. Building a 10x experience from that baseline is easy because the bar is so low and legacy companies have very little consumer product expertise. Thanks to tools that make it way easier to prototype, you’ll see workers test out their own concept tools to solve their own individual pain points and then try to sell it.

- Docs, nurses, billers, brokers, etc. are hypernetworked now thanks to social media/online communities. A recommendation from a peer here goes a really long way.
- AI can now do so many things that you can build easy-to-try apps/tools that people can just get started with and immediately handle a process that is a huge pain in the ass for them. They can log into portals, read documents, make calls, fill out forms, and other tasks that take up a huge amount of time in their day. All from a mobile app, chrome extension, and more.
- Business models are making this sustainable in the form of free + advertising, de-identified data sales, affiliate links, or premium features. This can undercut enterprise pricing and make versions that individuals can afford or try out themselves.
Let’s look at an example in OpenEvidence, and talk about opportunities in other areas.
Quick announcements - FINAL RUN OF EHR COURSE!!!
I’ll stop bothering you about courses (when I’m dead), but just wanted to give you a heads up that TODAY IS THE LAST DAY YOU CAN SIGN UP FOR OUR EHR COURSE (FINAL RUN). If you need to analyze EHR data or use it in your ops, this is the course for you. There’s lot of weird traps you can fall into if you’re not careful
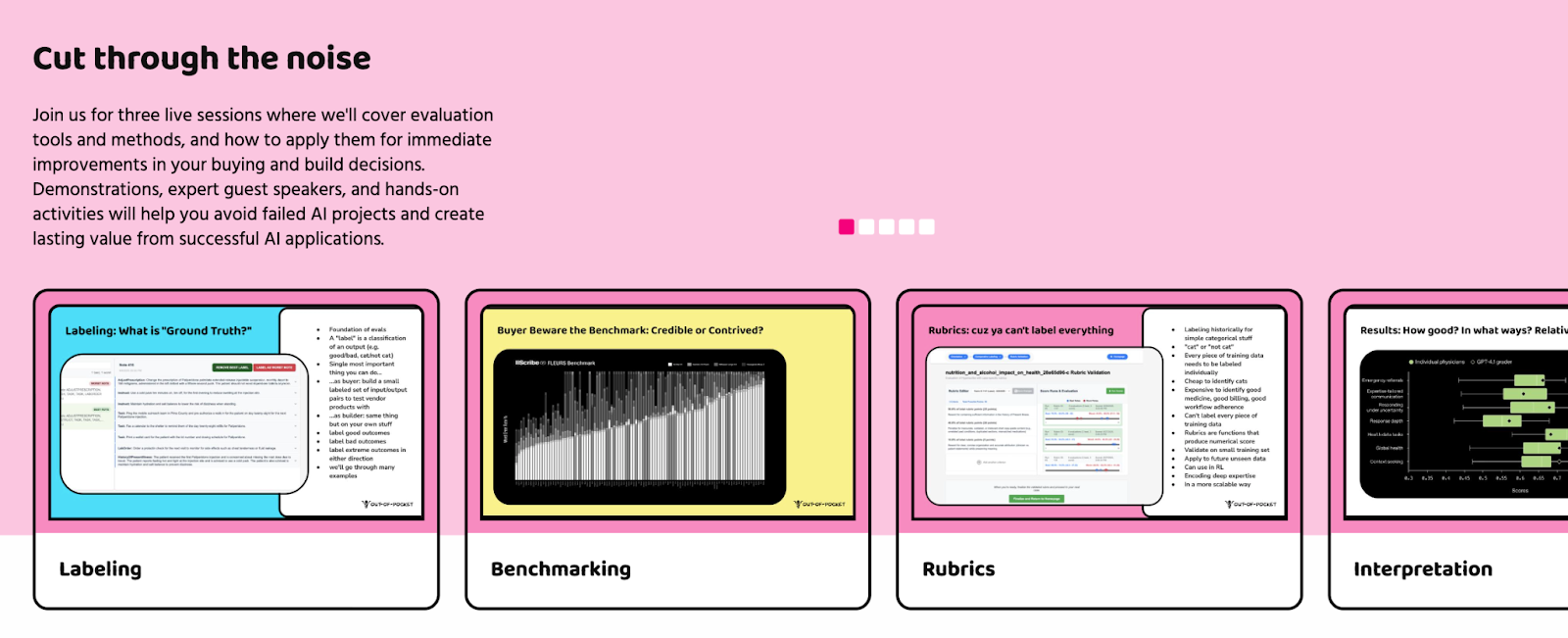
And don’t forget we have a FREE course starting 10/28 with Canvas around how to evaluate AI products. We’ll talk about some of the main areas of evaluation and go through some case studies that you might see in the real world
And if you like free courses, ANOTHA ONE (are we still making that reference?). We’re partnering with Navina to talk about value-based care operations and how AI is doing some interesting stuff here.
It’s also free, come through.
Back to the show…
{{interlude 3}}
What OpenEvidence Has Shown Us
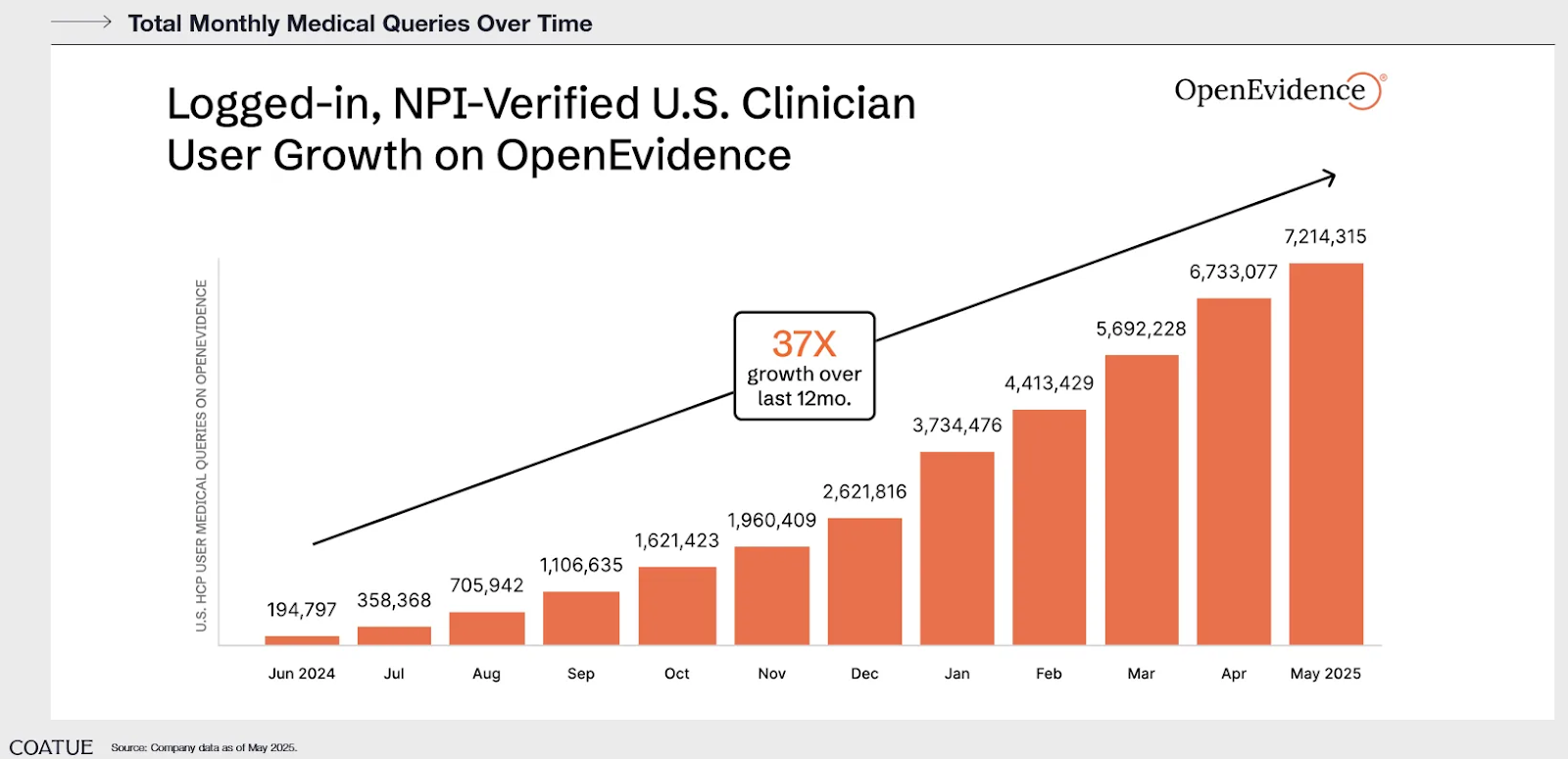
It’s been cool to watch the rise of OpenEvidence as a company. It’s been uncool as a person who invests in health tech and missed the one company that’s doing well. This qualifies me to raise a healthcare fund.
For those who don’t know, OpenEvidence is essentially a medical information search with a chatGPT-like interface. They guardrail and cite responses to the New England Journal of Medicine (NEJM), JAMA, etc. OpenEvidence is one of the few times in healthcare you see true product-led-growth and word of mouth adoption between clinicians. Usually that only happens when someone brings doughnuts to the office.
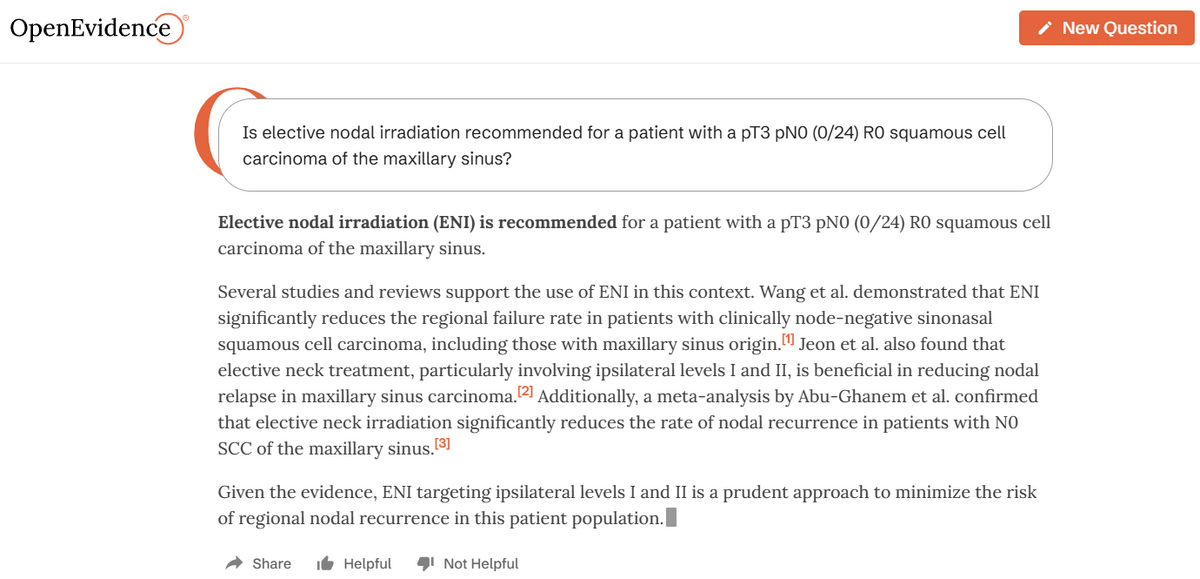
There are two interesting parts of OpenEvidence that are related to each other. The first was their choice of using a bottoms-up approach for distribution. Rather than try to sell this as a tool to hospital systems, they basically just put it on the App Store for free and people started downloading it. Then doctors started telling each other, people at NEJM started using it, and the rest is history.
It was a very explicit choice to not do the top-down sales motion, which is what virtually every other digital health company has done.
“…had we taken a top-down approach, had we taken an enterprise SaaS approach and been in waiting mode for meeting number 17 with the hospital system and no one was using it, well, if no one was using it, that would include no one at the New England Journal of Medicine using it, which would have meant that they wouldn’t have fallen in love with it, which meant that we would have never had an opportunity to strike a content partnership with them that would have been it…
In our case, the whole thing was a virtuous cycle. We put it out there, people downloaded it for free.” - Daniel Nadler, OpenEvidence CEO
The second is that instead of trying to immediately monetize from institutions, they seem to be targeting a free model that monetizes through advertising (acquiring Amaro). Looking at their privacy policy, I’d guess they also (or plan to) sell de-identified query trends to different companies and send target paid surveys to docs. You can tell how much time I have on my hands if I’m reading the privacy policy.
This is very different from traditional enterprise SaaS sales. It means that your goal has to be hooking consumers to your product for long periods of time. In a traditional enterprise software sale your goal is to keep your buyers - the administration - happy on the metrics they care about. Things like price, the ability to track productivity of employees, and increasing the size of the committees needed to pick these tools so everyone looks busy.
Plus in a traditional enterprise sales you’re in a chicken and egg situation where you can’t really charge much until you demonstrate value, and you can’t demonstrate value until you’re deployed at the enterprise. In a free with advertising model, you get more flexibility because you can immediately get users and figure out how valuable your product is.
How I’m thinking about opportunities for front-line worker tech
The growth of OpenEvidence has me excited about the future of applications that go directly to employees, circumventing enterprise sales. These are tools that are so useful that employees will just get it themselves.
A few heuristics I’m now using to look for opportunities:
First, what is an example of a task that should be done at the point of care that today requires a frontline worker to go to a computer or another room? AI makes the phone and Apple Watch user interfaces much easier to use. You can use one app with ChatGPT instead of needing to chain searches on mobile which sucks. Voice dictation is now way better in a way that it can actually be understood and useful in hands-free situations, etc.
OpenEvidence is a good example - clinicians were going back and forth to their computers to check UpToDate, and complex querying across the mobile app was a chore.
Second, where are areas that an employee has to ask someone else with expertise for a quick ask? This could be going to another clinician with expertise in a specific area, drug, etc. This could be going to someone with technical skills for a quick task or data pull, etc. AI is particularly good at being an “expert consult” and doesn’t get annoyed when you swing by for the 10th time in a day.
For example, InPharmD (disclosure: investor) lets clinicians get more information on drugs that they would normally ask a clinical pharmacist for help on. This is usually triangulating their own drug expertise with an understanding of the local hospital ops (e.g. what’s in inventory).
Finally, what is an example of something that healthcare workers are doing non-compliantly but it’s so helpful they’re doing it anyway?
If you look across frontline healthcare workers (pharmacists, home care workers, clinical research coordinators, etc.) you can probably find a lot of …questionably compliant things that people turn a blind eye to because it’s helpful for the patient and their workflows. Could you create a version of X behavior that IS compliant?
AI in particular has opened this door for obvious reasons. Are people voice dictating in places they shouldn’t? Or putting patient info in LLMs that they shouldn’t? Or sending photos, screenshots, docs, and patient info into group chats? I know the answer is yes, I’m just not a rat.
There’s going to be more scrutiny into how data enters and exits healthcare companies, so there’s probably an opportunity to enable these workflows in a more compliant way.
Some examples where there might be opportunity
Let’s take a few examples from a few different types of employees/frontline workers in healthcare and where there might be opportunities to build tools directly for them.
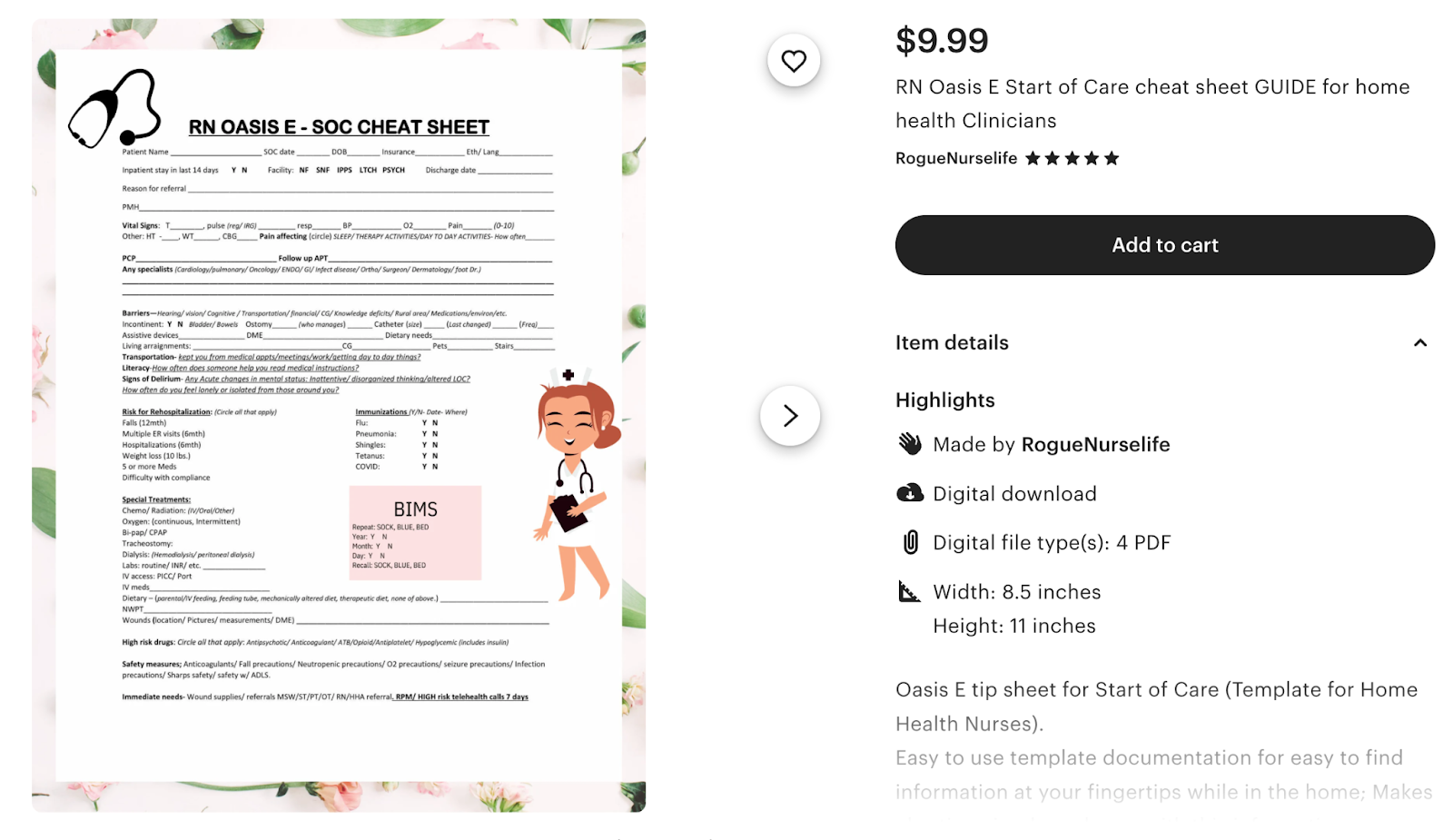
- Home caregivers/aides/nurses - They have to document a million things to get reimbursed. Clock-in and clock-out times, take photos and videos of patients to log tasks you helped with, monitoring the patient to see if they need to be escalated. Who’s using video pendants or voiceAI to track this passively and turn it into documentation? People on reddit are already doing this online with voice-to-text. Who’s using voice bots to call and schedule appointments for patients on behalf of the caregiver?
- Clinical research coordinators (CRCs) - there’s so much of this job that’s logging into portals and filling this out, moving data from point A to point B, or logging what happens during a visit somewhere. What about an AI scribe for CRCs that collects data and logs it into the Electronic Data Capture (EDC) system? Or a chrome extension that watches you do the data input once, and then does for you going forward? A ton of the job is also calling patients and coordinating them, could that be a voiceAI bot they guide?
- Pharmacy Technicians - There’s lots of mobile apps already for pharmacy techs to keep up to date with drug information like Pyrls, Pocket Pharmacist, etc. so they can check drug info without needing to use the computer every time. But so much of what goes on in a retail pharmacy are visual checks for things in different rooms to make sure things are correct (right number of pills in the bottle, checking orders on screen, etc.) and then confirming it with things on the computer screen. Can a mobile app scan an insurance card, scan a bottle to give drug info, make smart substitutions, and quickly generate letters explaining the substitutions?
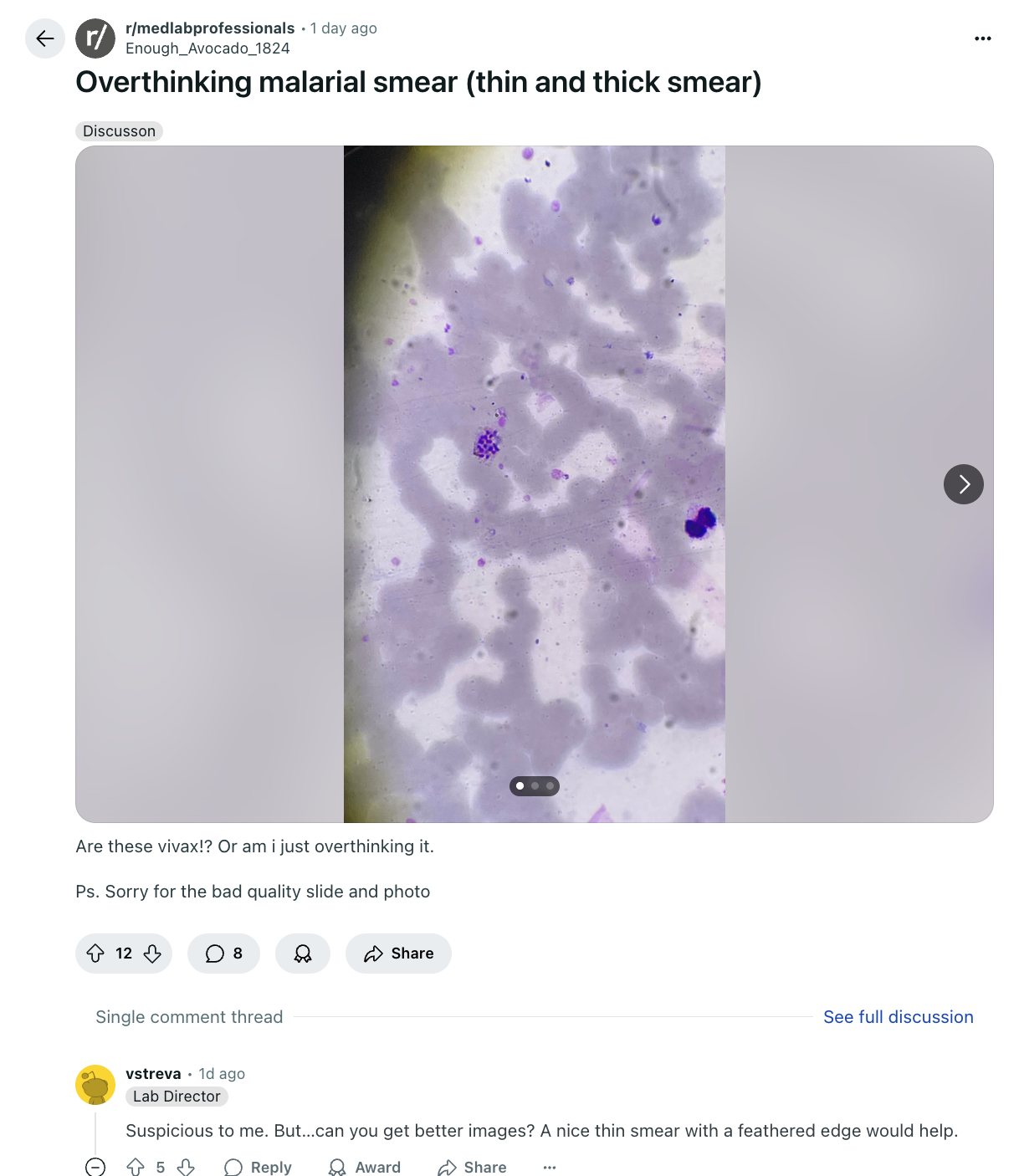
- Med Lab Technicians - The med lab has a lot of situations going from gloves on, to gloves off and documenting things. Could you use voice to document and control machines? LabVoice seems to be exploring something like this. Or frequently you see people in the lab subreddit ask to get second pairs of eyes on some test they’ve run, can LLMs be a second opinion in the pocket?
You can go through this exercise with a TON of different employees in healthcare. Either go on the subreddits/facebook groups where they congregate, or watch “day in the life” videos of a given role (e.g. here's one about a pharmacy technician).
Parting Thoughts - The OpenEvidence Story Continues
While I think OpenEvidence has done a great job so far, the party is just getting started. There’s a few things to watch that will shape future opportunities in the direct to employee space:
What does competition look like? Competitors like Doximity and UpToDate have launched similar products in this area. In addition we’re starting to see overlap between other “consumer first” products like AI scribes (with OpenEvidence launching their own too). There’s clearly going to be some convergence around scribing, clinical decision support, and literature search in one product. This raises a few questions around how much an existing brand matters here, and also whether clinicians care about the knowledge base and sources that these tools are built on top of. One of the main things people like about UpToDate is that it’s curated by docs at top hospitals, does that still hold the same weight?
What will the employee tolerance look like for incorrect answers? With any AI tools in the direct-to-employee space, there are going to be times when it’s wrong or hallucinates. In OpenEvidence’s case it’s no different, the wrong answers come up in doctor subgroups all the time. Currently we are more comfortable with humans ingesting information and occasionally getting it wrong but have way lower fault tolerances for AI doing that. I’m interested in how direct-to-employee tools position mistakes since employees might not care about it in the same dimensions that enterprises do.
How will the business model and pricing play out in this space? OpenEvidence free tier looks attractive compared to UpToDate which is $500+/year for an individual. But how will this look as these companies need to get more deeply integrated with EHR data and the rest of the enterprise software stack? Will they need to eventually charge enterprises and provide an ad-free alternative?
- An interesting subpoint to this brought up by Chethan Sarabu. Enterprise pricing models like licenses per seat end up creating bad user experiences. For example requiring increasingly more complicated logins and connecting to the right wifi network to make sure you can accurately track the number of seats being used. Will companies doing bottoms-up adoption find different types of enterprise pricing that don’t create bad user experiences?
- I’m curious to see whether there’s eventually bigger backlash in the physician community around pharma ads at the point of care. It’s possible you’ll see pushback on the kinds of advertisement allowed - which might make the economics more difficult (though there are definitely other buyers for that kind of ad slot).
How big of a business can direct-to-employer tools become? If doctors are your users, you have eyeballs that are extremely valuable that companies will pay a lot of money for. When you pick other employee types and get increasingly more niche in the pain points being solved, how big of a business can those be? I think these can also be interesting cash generating side hustles too!
How will the fight with security and compliance play out? In this situation employees are using tools outside of what the enterprise gives them. But enterprises HATE having parallel shadow IT happening inside their hospitals. Part of the bet here is that the tools are so loved that compliance is forced to figure out how to make them work internally. But another version is that instead enterprises clamp down on these apps instead and find ways to make it difficult to use them.
Hardware? Does new hardware for employees open new avenues? For example, there are lots of clip-on pins like Plaud, Limitless that you can talk to AND record your surroundings. Does this unlock new use cases for people? How about something like the Meta Smart Glasses that can see what you see and guide you? This feels especially helpful in areas you’re hands-free and need a screen for guidance. Or what about miniaturized medical devices like Butterfly’s ultrasound - are there other direct-to-clinician tools here? Hardware is definitely a harder business model, but also way stickier if people actually use it. Maybe healthcare employees will buy their own mini-hardware toys to make their lives easier.
I’m excited that companies are finally seeing a way to build businesses that are designed for the users in mind. If you’re building something here (especially for some of the more niche workers in healthcare), let me know!
Thinkboi out,
Nikhil aka. “Face Down, Bottoms Up (Adoption)”
P.S. We're announcing our Knowledgefest sponsors this week - if you're trying get in front of healthcare ops people hit us up.
Twitter: @nikillinit
IG: @outofpockethealth
Other posts: outofpocket.health/posts
{{sub-form}}
If you’re enjoying the newsletter, do me a solid and shoot this over to a friend or healthcare slack channel and tell them to sign up. The line between unemployment and founder of a startup is traction and whether your parents believe you have a job.
Interlude - Apply to Knowledgefest! And healthcare 101 starts next week!
See All Courses →Don’t forget the application for our Knowledgefest, our healthcare software engineering conference IS LIVE.
If you work in healthcare ops, you want to be here. This is where you learn playbooks, see what other ops people are doing, and build your network. It’s year 5 and we sell out every year - applications are due end of month.
And if you feel like you really need to get up to speed on how healthcare works, then you should let me teach you at Healthcare 101starting next week!This is for anyone hiring teams of non-healthcare people that need to get up to speed quickly (in 2 weeks) - we do group discounts too hit up ya boy. You’ll even learn how to make memes.
.png)
Get Out-Of-Pocket in your email


