




It’s the time for wearables
Get Out-Of-Pocket in your email
Looking to hire the best talent in healthcare? Check out the OOP Talent Collective - where vetted candidates are looking for their next gig. Learn more here or check it out yourself.
 Hire from the Out-Of-Pocket talent collective
Hire from the Out-Of-Pocket talent collectiveHealthcare 101 Crash Course
%2520(1).gif)
Featured Jobs
Finance Associate - Spark Advisors
- Spark Advisors helps seniors enroll in Medicare and understand their benefits by monitoring coverage, figuring out the right benefits, and deal with insurance issues. They're hiring a finance associate.
- firsthand is building technology and services to dramatically change the lives of those with serious mental illness who have fallen through the gaps in the safety net. They are hiring a data engineer to build first of its kind infrastructure to empower their peer-led care team.
- J2 Health brings together best in class data and purpose built software to enable healthcare organizations to optimize provider network performance. They're hiring a data scientist.
Looking for a job in health tech? Check out the other awesome healthcare jobs on the job board + give your preferences to get alerted to new postings.
This episode of Out-Of-Pocket is brought to you by…
Nikhil built Out-Of-Pocket into a 30,000+ subscriber healthcare media company. Behind the scenes, an Oceans Talent operator helps run the business, from systems and automations to the operational follow-through that keeps everything on track.
AI-fluent, proactive, and embedded in your workflow from day one. The result: a leaner team that can move faster.
—
Want to talk about sponsorship? Let’s chat, we have a bunch of ways we can work together and it doesn’t need to be me talking in third person.
So…what’re you wearing?
I’ve been talking to Samir Akre-Bhide and Afnan Tariq about wearables for a while now. Both of them have been seeing firsthand how wearables are changing screening and monitoring, but also have certain limitations in deployment. Samir brings the academic expertise, Afnan brings the clinical, and I am sick nasty with the pen.
At OOP, we’re all in on the healthcare x hardware intersection. That’s why we’re doing our hackathon this weekend (DEMOS IN SF ON SUNDAY 4/19!!!). Today we wanted to talk about WHY this area is particularly interesting today and what trends we should think about. This is a blended perspective of all three of us like some weird Indian hydra, but we’ll use the first person perspective for simplicity.
This is a two part series. Today in part 1 we’ll talk about the opportunity in wearables, and in part 2 we’ll talk about the challenges that need to be addressed. Sign up to get both parts. Or not if you prefer to stay unenlightened.
–
What makes wearables interesting
My Whoop showed me how dramatically alcohol negatively impacts exercise recovery metrics, but it also suggested 1-2 drinks has almost no effect on recovery. And yet it can’t quantify how good the hang becomes when that second cold beer hits my hand.
Most of the time I don't find my wearable data actively useful. But that changes when there's a layer of clean, reliable data AND I have a hyperspecific question. A 3am heart rate spike made me suspicious that my CPAP mask wasn't fitting properly while I slept. I found the issue, fixed it, and immediately improved my sleep quality.
That experience captures both the promise and the problem. Wearables generate enormous amounts of data. The question is whether anyone knows what to do with it.
Let’s start by talking about what makes wearables interesting and where we see promise today.
{{interlude 3}}
Regulation and reimbursement
Regulation and reimbursement for wearables has been a huge barrier to integrating them into healthcare. Why go under the additional scrutiny of being a medical device if you’re not sure how you’re going to make more money? But it does seem like things might be changing.
For a long time, the line was simple: if your device tracks heart rate for fitness, you're a wellness product. But in January 2026, the FDA basically reversed course and announced looser regulation of digital health products. The updated guidance now says whether a wearable is a medical device depends on how it's marketed, not whether the metric it measures could theoretically be associated with a disease.
On the reimbursement side - we started seeing remote patient monitoring (RPM) codes that suggested wearables would get paid for. RPM was fine in theory but in practice it was a mess. The model basically paid providers for collecting data rather than doing anything useful with it. That job is reserved for product managers. As you can imagine, payers have started fighting back against RPM.
Instead this administration seems to be testing a trifecta of changes to make it more attractive for wearables in healthcare:
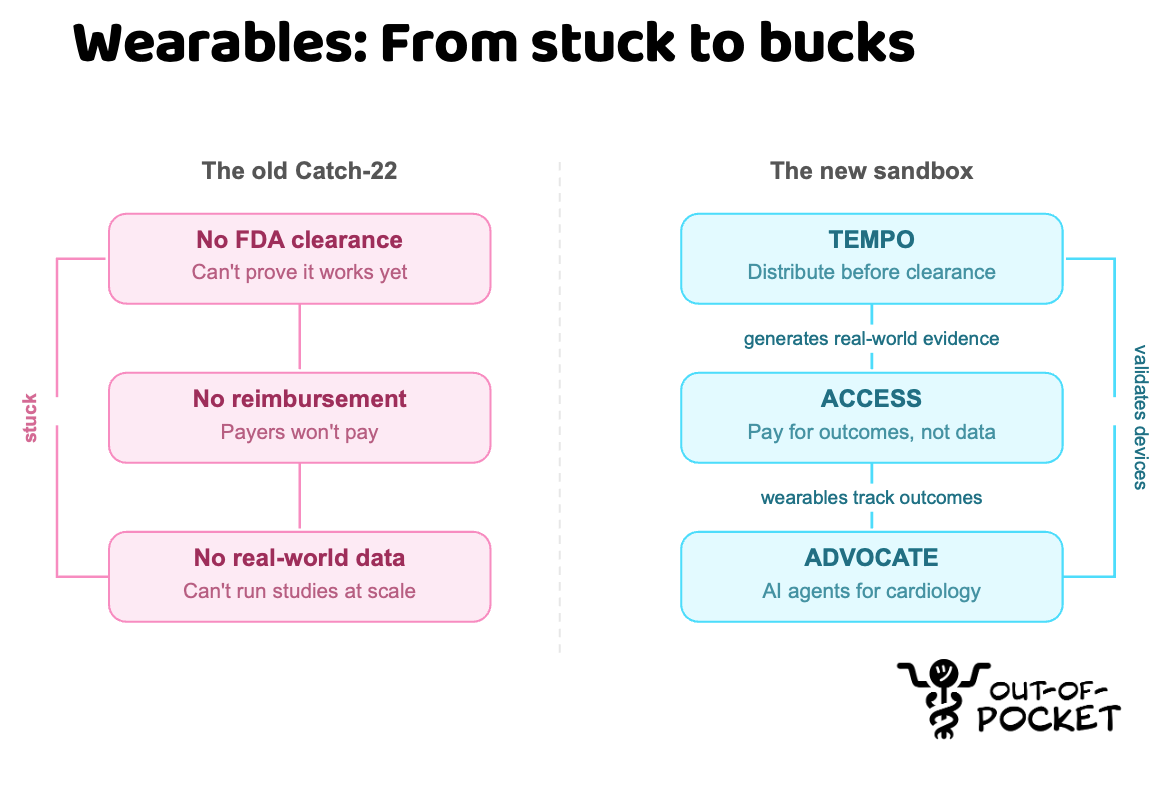
Payment: The new ACCESS model from CMS pays providers based on whether the patient's health actually improves. Things like blood pressure going down, diabetes being managed, etc. You’ll inevitably need wearables to track this and intervene with patients.
Regulation: The TEMPO pilot lets up to 10 digital health device manufacturers distribute products under FDA enforcement discretion. This means they can distribute before full clearance as long as they're generating real-world evidence within ACCESS. That breaks the old Catch-22 where you couldn't get reimbursed without FDA clearance and couldn't get clearance without real-world data. Now there’s a sandbox to play in.
Technology: the ADVOCATE program from ARPA-H aims to use AI agents to autonomously provide cardiology care to patients. This is viewed as an engineering problem to be solved, and wearables are a key part of solving this as the ARPA-H team has specifically said.
“Further, data inputs from wearables such as heart rate, blood pressure, and the EKG add significant value to the care of these patients, yet wearables tend to be sidelined in routine clinical practice. - Haider J. Warraich, STAT News
We’re about to create god out of silicon, and I’m still going to ignore it when it tells me to cut back on the salt.
R&D: ARPA-H also launched the Delphi program to fund next-gen biosensors. The idea is modular "chiplets" that can be mixed and matched into wearable or ingestible devices. Delphi wants devices that can track hormones, inflammatory markers like cytokines, and drug levels continuously. The program runs 4.5 years with prototypes due in 2 years, so we’ll actually be able to monitor if your cortisol levels spike when you’re framemogged.
–
I’m cautiously optimistic, but it does seem like the regulatory regime around wearables is changing.
We now track diseases from a healthy baseline
In most healthcare contexts you start measuring metrics related to your disease once you’ve been diagnosed or in an at-risk category. What makes wearables interesting is that people are wearing them starting from a healthy baseline. If I develop Parkinson’s in 10 years, what does my Apple Watch data show about how dyskinesia actually developed? Has my heart always skipped a beat when I see my wife, or is that an arrhythmia? This might tell us more about when diseases actually start and push us to intervene earlier.
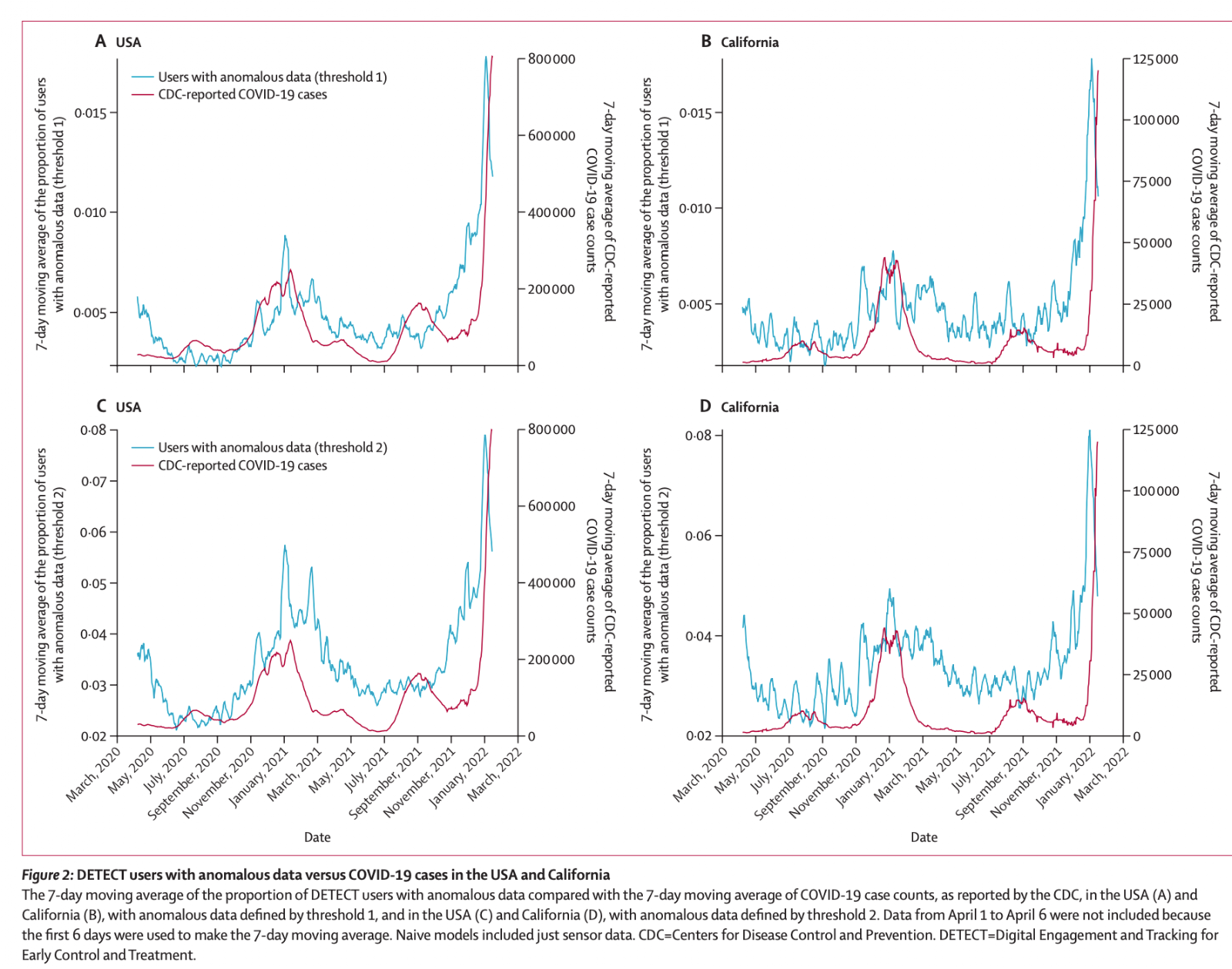
COVID was actually an interesting testing ground for this because it was novel and the episode was short. Multiple studies showed that wearables could detect infections several days before symptoms appeared by detecting deviations from each person's own baseline. A UCSF study using Oura rings could detect COVID an average of 2.75 days before diagnostic testing with 82% sensitivity/64% specificity. The Scripps DETECT study used Apple Watches, Fitbits, and Garmins for individual and population-level outbreak tracking.
Imagine how many other diseases we might be able to intervene on if we’re studying more people starting from when they’re healthy. We can test new interventions, enroll people earlier into trials by detecting them earlier, and potentially change the trajectory of a given disease.
New types of screening, standardized measurement, and disease subtypes
For many diseases that we test, we look at values in a single point in time. Wearables add temporality, looking at how all of those same values trend over many different contexts and longer time periods. This introduces new variables that can tell us more about a given disease. How your biomarkers change in a given time of day, or what is the slope of change in a specific period (e.g. how fast does your A1C spike then normalize when you eat).
This opens a few different doors.
- Disease subtyping - What we bucket into single diseases may actually be different subtypes and continuous monitoring can distinguish them. Take Parkinson’s for example. Here’s a paper that used wearable data to identify three distinct subtypes: a mainly motor/slow progression type, an intermediate type, and a diffuse/malignant type with much faster cognitive and motor decline. Patients with the diffuse/malignant phenotype were 8 times more likely to show rapid progression, so how you’d manage them would be very different.
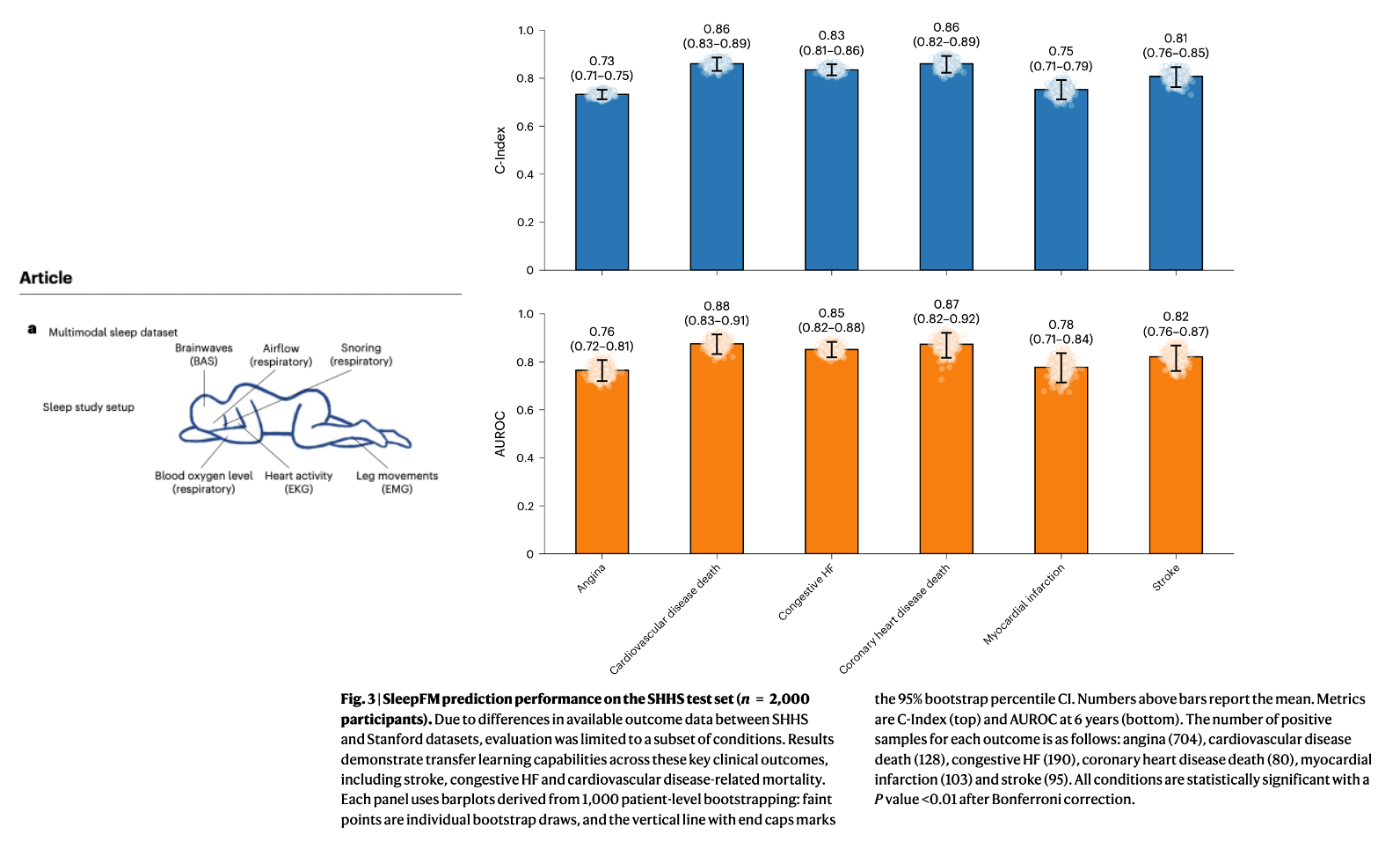
- Easier screening modalities - Can wearables make it easier to screen for diseases than the current standard? The SleepFM paper that came out recently is really interesting. It’s a foundation model trained on 585,000 hours of sleep data from 65,000 participants. From a single night of polysomnography (PSG), it seems to be pretty good at predicting over 130 health conditions (including dementia, heart disease, stroke, etc.). In particular the paper called out being as good as fMRIs at monitoring dementia, despite PSGs being much cheaper and more accessible.
- Objective measurement - Many of the disease scales we use today are subjective to the person administering it or filling it out. Epileptic patients need to track their seizures and they underreport. Two experts filling out the EDSS scales for multiple sclerosis frequently disagree with each other. And the scales used for mental health…they’re asking me if I feel anxious. Who the f*** isn’t feeling anxious, have you been online? Wearables could help provide more objective monitoring by looking at sleep, physical activity, body movements, and more.
Wearables are defensible in a commoditized consumer stack
The consumer health stack is commoditizing. Getting labs, pulling in your medical records, booking a telehealth visit, even AI primary care. All of these are relatively swappable and like VC cash incinerators by themselves. When every layer of the stack is interchangeable, you start asking which piece actually has staying power.
I think it's wearables, and one core reason is body real estate. You're not wearing two smartwatches. You're not rocking an Oura Ring AND a Samsung Galaxy Ring AND a RingConn like some kind of biohacking Xiaolin Showdown. You pick one. And once you've got 18 months of resting heart rate data and sleep baselines built up on that device, switching to a competitor means starting over from scratch.
Plus every other piece of the consumer health stack is reactive and requires you to initiate. You have to book the visit, order the labs, log into 15 different MyChart instances to pull up the records. Wearables can alert you proactively and say “something’s off”, as my Oura ring does every time the GERD dragon rises at night.
And ironically, I think the business model for wearables is about to become more valuable. Software companies are currently going through an existential crisis realizing that they might be getting commoditized as AI gets better at engineering and many of the moats they’ve been used to are evaporating. Hardware has always been shit on because they have worse margins, they’re hard to scale, and there haven't been network effects. But now this might be changing - wearable companies get margins from the hardware AND recurring software (Whoop's subscription model, Oura's membership, Apple's ecosystem lock-in). Plus the moat is stronger as people build

—
Featured Jobs
Some companies are hiring!
Parakeet Health - Customer Success Manager (SF, In-Person)
- Healthcare still runs on hold music and fax machines. Our AI agents handle calls, faxes, and patient outreach for practices across all 50 states -- automating the most tedious admin tasks. We're hiring CSM #2 to help practices transition to this agentic world. Lean, ambitious, and AI-pilled team. Apply Here.
Yuzu - Software Engineer (New York)
- We’re the only TPA that built our claims software in-house from day 1. We handle >$1M in payments daily at the healthcare/fintech intersection. Hiring engineers at all levels. We’re not AI or SaaS, we run ops in-house to de-risk engineering. We value honesty and responsiveness. Apply here.
Double Blind Bio - Founding Engineer Lead (San Francisco)
- Cut clinical trial timelines in half. $7M raised from top-tier VCs, 200+ sites live, pharma design partners signed. Join a founding team of life sciences + AI veterans as a senior team member who ships full-stack on agentic systems, wants to be a player-coach and grow a team. Email careers@doubleblindbio.co
Conclusion and a pretty crazy very related story
Afnan just went through a real-world scenario where a wearable was extremely helpful. He was literally reviewing this piece on a plane when someone asked if there was a doctor on board. One day they’ll ask if there’s a newsletter writer, I’m sure of it.
There was a woman that was pale, clammy, unresponsive, eyes glassed over, completely out. He checked her pulse at the carotid: flat 70, normal. He had to rule out syncope, seizure or worse. They grabbed the plane's wrist cuff for blood pressure which was 154/140, obviously incorrect (NK note: uh yeah…totally).
With 90 minutes left in the flight, he needed to figure out if she was stable or if they were going to divert the plane somewhere over New Mexico. He asked if they had a portable EKG but they did not.
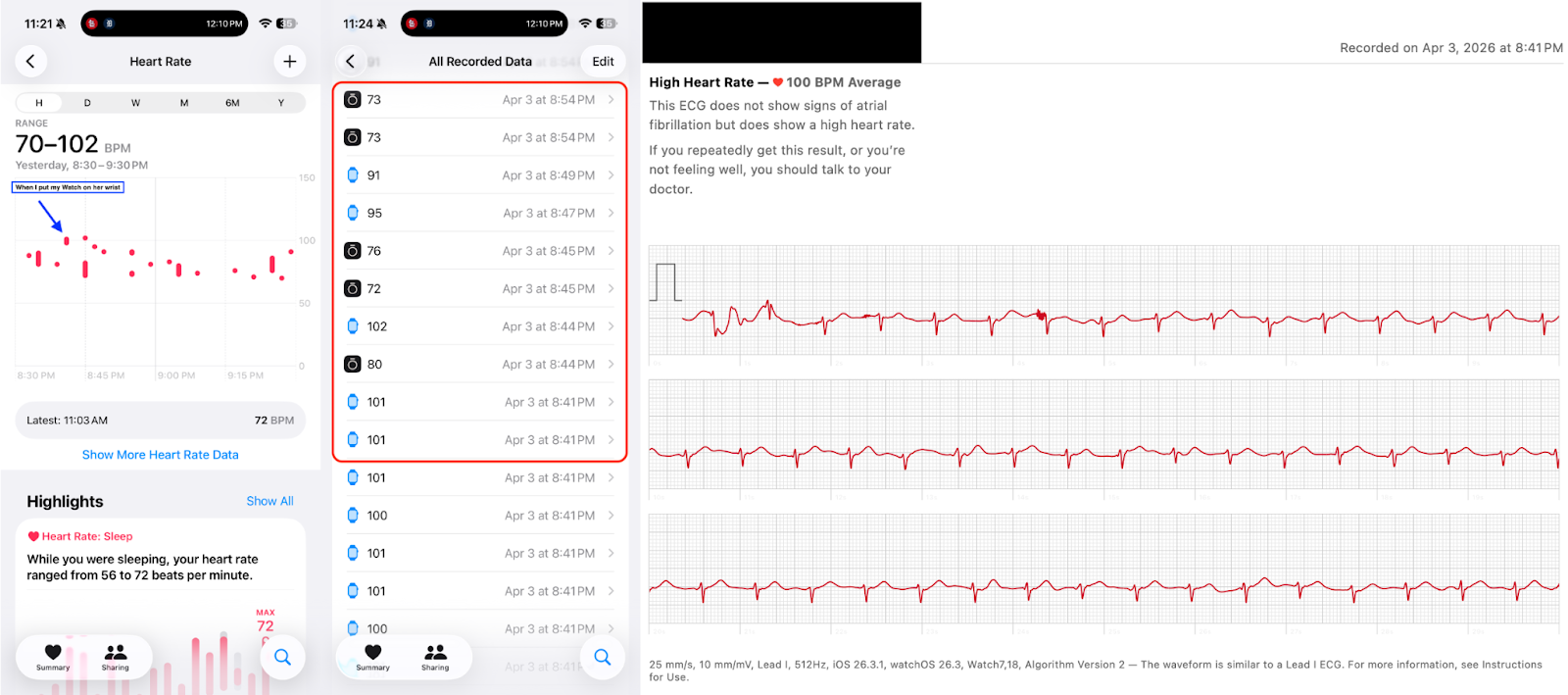
So he used the Apple Watch that he was already wearing! He took it off his wrist, put it on hers - and had her take an ECG and it was sinus rhythm, 100 bpm. He sat down a couple rows ahead and tracked her heart rate on his watch from his seat where he watched it come down from 102 to 95 to 90. He was also wearing an Oura ring, so his iPhone was simultaneously logging his heart rate and hers. Accidental dual-patient monitoring. (Afnan said something about flow state - comparing this to being like Patrick Mahomes in the playoffs where his HR spiked more when he didn’t have the ball in OT than when he did. Yes, Afnan…sure)
Eventually she stabilized and the story had a happy ending. Afnan got back to his seat and in an incredibly meta moment, added this story to the end. And added a comment saying I needed to get a copy editor.
Stories like this show us that wearables have a lot of promise when we know how to use them to their fullest. But there’s still a lot of issues with them that we need to fix in order to reach their potential. In part 2 we’ll go through them, sign up to get it.
Thinkbois out,
Nikhil, Samir, and Afnan aka. The Wearable Ravana
Twitter: @nikillinit
IG: @outofpockethealth
Other posts: outofpocket.health/posts
If you’re enjoying the newsletter, do me a solid and shoot this over to a friend or healthcare slack channel and tell them to sign up. The line between unemployment and founder of a startup is traction and whether your parents believe you have a job.
Interlude - Apply to Knowledgefest! And healthcare 101 starts next week!
See All Courses →Don’t forget the application for our Knowledgefest, our healthcare software engineering conference IS LIVE.
If you work in healthcare ops, you want to be here. This is where you learn playbooks, see what other ops people are doing, and build your network. It’s year 5 and we sell out every year - applications are due end of month.
And if you feel like you really need to get up to speed on how healthcare works, then you should let me teach you at Healthcare 101starting next week!This is for anyone hiring teams of non-healthcare people that need to get up to speed quickly (in 2 weeks) - we do group discounts too hit up ya boy. You’ll even learn how to make memes.
.png)
Get Out-Of-Pocket in your email


