




Do you need a doctor leader at your healthcare startup?
Get Out-Of-Pocket in your email
Looking to hire the best talent in healthcare? Check out the OOP Talent Collective - where vetted candidates are looking for their next gig. Learn more here or check it out yourself.
 Hire from the Out-Of-Pocket talent collective
Hire from the Out-Of-Pocket talent collectiveHealthcare 101 Crash Course
%2520(1).gif)
Featured Jobs
Finance Associate - Spark Advisors
- Spark Advisors helps seniors enroll in Medicare and understand their benefits by monitoring coverage, figuring out the right benefits, and deal with insurance issues. They're hiring a finance associate.
- firsthand is building technology and services to dramatically change the lives of those with serious mental illness who have fallen through the gaps in the safety net. They are hiring a data engineer to build first of its kind infrastructure to empower their peer-led care team.
- J2 Health brings together best in class data and purpose built software to enable healthcare organizations to optimize provider network performance. They're hiring a data scientist.
Looking for a job in health tech? Check out the other awesome healthcare jobs on the job board + give your preferences to get alerted to new postings.
New Discussion Post - The Doc At A Startup
I can feel the knives coming out just writing out the title of this one. I somehow got ratio’d on LinkedIn yesterday just saying I was going to write about this. I didn’t even know that was possible on a professional social network.
There seems to be a pretty big disconnect when I talk to people about whether you need a clinician or not when you’re starting a health tech company.
I think we manage to do a pretty good job of nuance in this newsletter and readers send in great points. So this week’s question is…When do you need a clinical leader? How do you think clinical leaders should be chosen/vetted/set up for success? Any stories about when it did or didn’t work out.
Email me your responses and I’ll post a few of my favorite responses next week (anonymous if you want).
A few of my thoughts below. Just a reminder that I have no idea what I’m talking about and don’t feel strongly about most of the opinions below, so you can change my mind!
Quick note - Final run of courses!
We have a few courses that are doing THEIR FINAL RUN EVER. If you ever wanted to take an OOP course or use your education stipend on something you might actually find useful instead…here you go. Email sales@outofpocket.health for group discounts
- Selling to Health Systems (starts 10/6) - If you need to sell to hospitals, you can’t just like…show up. We’ll teach you how to sell to hospitals the right way, which include assignments to refine your pitch. ENROLLMENT ENDS NEXT WEEK.
- EHR Data 101 (starts 10/14) - Hands on, practical introduction to working with data from electronic health record (EHR) systems, analyzing it, speaking caringly to it, etc.
- Claims Data 101 (starts 11/10) - Practical introduction to claims. Ideal for all healthcare backgrounds, this course covers what claims are, why they exist (WHY GOD), and how to most effectively use them.
Also separately…if you work at
- Banner Health
- Baylor Scott & White
- Bon Secours
- IQVIA
- HCA
- Molina
And want to come to a kinda secret AI event we’re hosting in NY this fall, email alex@outofpocket.health.
Back to my skewering.
{{interlude 3}}
Why is “should we have a doc in leadership” a tough question?
At first glance it would seem like the obvious answer is “of course! How could any team in healthcare not have a clinician on the leadership team?” I would love to live in this fantasy ideal world with abundant energy, no human suffering, and trees that grow clinicians willing to take pay cuts.
But since we want to have an honest discussion of this, we should look at the practical tradeoffs.
The first and most obvious is cost. The opportunity cost for a doctor’s time is extremely high and unfortunately equity to offset that isn’t as appealing. Doctors already waited like 40 years to get their first real paycheck, even they have limits.
This makes hiring a doctor usually an extremely high cost hire which increases burn rate significantly. This can be more tolerable at mid/late stages, but might be tough if you’re just starting.
The second is figuring out what role you want a clinical person to fill. At baseline, they bring expertise in their area of practice, and (usually) the necessary professional license to see patients. Are they going to be seeing patients? Do you need them for sales/BD connections? Do you need them getting in the weeds with the tech team? Depending on your specifications, that pool can become much smaller.
Third is whether you’re at the right phase of needing them. If you don’t have a high volume of patients yet or you only have a few pilots at some hospitals and the amount of clinical input you need is sporadic, it might not make sense for there to be a full-time clinician at your company. If you just got a contract and need to fill the role ASAP, it’s also easy to hire a doc that’s a bad fit out of desperation. Now you gotta eat an apple a day smh.
The final and maybe most important is that having a doctor on your team doesn’t always solve the problem.
- Your doctor might not have deep experience in the specific problem you are trying to solve (e.g. different subspecialty, hasn’t done complex chronic patients, not used a modality like telemedicine).
- Ask ten doctors for their opinion on a clinical problem, and you’ll get ten opinions (plus a fatass bill). Docs make lots of judgment calls, and there could be a ton of variance on what they prefer, so a singular clinician’s input on your product still doesn’t reflect what will be successful in the market.
- The clinical person on your team hasn’t actually practiced in a while or at all. They’re more of the “MD/MBA I realized I didn’t want to go into residency” type and aren’t tuned in to the actual day-to-day clinical workflows.
- You have a doctor in leadership in order to help sales but your end buyer’s concern isn’t related to whether you have clinical expertise or not.
- The clinician is running away from medicine and looking for anywhere to land instead of actually excited to work at a startup.

As the company grows and gets more resources, you’ll have more flexibility and the ability to bring clinical folks into leadership positions. Even then, many companies wonder if they should hire clinical leadership for their specific company needs.
When is it a must-have vs. nice-to-have?
If you acknowledge the practical reality that not every single healthcare company will have clinical leadership, then you gotta triage which companies really should have it vs not. I guess this is now a startup emergency department.
Here are my 2 cents on when clinical leadership is a must-have vs. nice-to-have, and I am very open to changing my mind on this so send me your thoughts.
Clinical leadership is nice-to-have
- You are handling a back-office process that doesn’t touch the clinical or patient side of things (e.g. credentialing, revenue cycle services, filling out RFPs, value-based care contracting, etc.)
- You are selling software or analytics tools to people that deliver care but your company itself does not (e.g. databases, analytics, patient engagement tools, etc.)
- You do something unrelated to patient care at all (broker/benefits stuff, compliance, staffing, supply chain/inventory, etc.)
- You are not in healthcare, then why the f*** have you read to this point?
Clinical leadership can start part time, but a must-have once you grow
- Your main buyer is a medical persona of some kind, even if you’re selling a back-office tool. At a certain point it’s important to the success of your business that someone can talk “doc-to-doc” (trauma bonding sales).

- You have a medical owner of a Professional Corporation (PC). You can rent this out for a while, but at a certain point it’s going to become expensive to keep renting + the complexity will increase. You’ll want to have someone in-house at that point.
- You have frontline clinicians that cannot practice alone (e.g. nurse practitioners, medical assistants, etc.). You can usually have someone fractional for oversight as you start.
- Once you have at least 5+ people delivering care to patients on behalf of your company you should have a full time person in charge of overseeing your care team. [Would love to hear other opinions on this]
- This is true for low complexity care, but for high complexity care you will probably need someone full time on your leadership team from the start.
Clinical leadership is a must-have from the start
- You are trying to deliver a very new care model of some sort. If you are building a unique care protocol, you should probably have a physician in leadership that’s co-designing it. They’re overseeing it, know when to adjust it, and understand the practical clinical challenges.
- This can be care delivery in a new type of payment model (e.g. some form of value-based care), this can be a greenfield area of care (e.g. longevity, deprescribing), or even new modality (e.g. primary care where AI handles all the patient intake and chart review).
- This is not an inherently clinical skillset, and typically requires someone strongly familiar with clinical ops who can understand how things like staffing, escalation, etc. will work.
- Your differentiation during sales/marketing IS a strong clinical culture. You’ll need a clinical leader that’s well-respected and can set that from the ground level. (You should be honest with yourself on whether a strong clinical culture matters in the slice of healthcare you’re tackling.)
- You are working with patients that have very complex care needs. Dual-eligibles, people with serious mental illness, etc. need more supervision. You should have a clinical person on your team from the very early days here.
- You are creating any sort of tool that is a new form of diagnostic, therapeutic, or triaging of patients. Hopefully I don’t need to explain why.
- You are selling to enterprises where they are going to ask who is the medical person overseeing that care protocols are being followed or will make the clinical judgment calls. For example, if you’re running clinical trials, doing a home care model, or you’re a payer of some kind.
Some potential alternatives
If you can’t afford to have a full time clinical person on your leadership team, there’s a few different axes to think about.
- What is the structure of the engagement? Full time, fractional, or advisor? Hourly rate, monthly retainer, equity, or a combination?
- What is the seniority and skillset of the person? Junior learning the ropes or senior that’s done X things for 30 different companies?
- What is the nature of the work you need done? The same thing rinse and repeat each week or you want someone who can help field a bunch of different things that come up.
When you think about it through these lenses you can get a few different arrangements.
One is a fractional medical director/CMO. In these situations you’ll typically pay monthly retainers or hourly rate with a minimum number of hours + maybe a small piece of equity in exchange for certain responsibilities and hours of involvement. There are a lot of docs that will do this for multiple companies and you pay way less than having a full time clinician on staff. You’ll also want to figure out upfront if this is a “join full-time once we grow” kind of relationship or if it’s purely a transaction for the time being.

Another option is having clinicians as advisors in exchange for just equity. This can be a great way to have people to provide clinical input on your product and provide credibility with buyers. They can also help with vetting full-time clinicians you bring on late.
However, a few warnings here.
- I don’t think I’ve ever seen a clinician take only equity and do anything like patient care or things that might put their license at-risk. That might exist but I’ve not seen it, and frankly you should be wary of someone willing to do that.
- Make sure you and the advisor mutually understand exactly what each other are getting from the agreement. You don’t want the advisor to get blindsided because they didn’t know they were going to be named in a proposal. One time I texted a doctor friend that was on a deck and he had no idea the startup had him in it.
- There are a lot of… “professional” advisors that basically just put their name on every startup in exchange for equity but aren’t involved at all. You might think you’re getting credibility by getting them, but everyone knows they aren’t actually involved with your company.
And then another tactic is to have customer advisory boards or advisory councils. Similar to having clinicians as advisors but usually smaller amounts with more physicians. Typically this is more about having ways to get input on your product from people you’re trying to sell to or "real-world" clinicians. It turns out that docs that opt to work at startups aren’t representative of the field (aka. they know how Google calendar works).
The advisory board structure can get you multiple clinical perspectives, but these aren’t clinicians who are going to take on risk on behalf of your company.
Figuring out which arrangement is right for you is more of an art than a science, which you should be good at since you dropped pre-med. For an early stage company who is trying to minimize burn and isn't doing something complicated, a full-time medical director (Director, VP, "Head of Clinical") might be better and more cost-effective than a fractional CMO.
Conclusion + random thoughts
A few random thoughts that are related to this topic.
- Clinicians and companies should both be vetting each other to answer the same question: what tradeoffs are you comfortable making between speed and quality when it comes to making clinical decisions?
- This is a spectrum that does not have a clear cut answer. Most of the miscalibration happens when company and clinical leadership don’t have the same framework for making those decisions. Not every decision will have the luxury of waiting for a randomized control trial, and you also can’t just vibecare for patients.
- The best way to evaluate this is by doing a bunch of potential scenarios that might come up at your company and see how you’d answer. We want to push X feature into production, how should we test it? We want to increase a doctor’s patient panel size by 10%, how would we get comfortable doing that? A patient has a medical issue because of a mistake we made for X reason, what happens next?
- Anecdotally I’ve heard that emergency medicine docs and docs that have typically worked in lower resource settings (e.g. federally qualified health centers) have an easier time transitioning into startups even if they’ve never worked in one. They get the pacing and tradeoffs aspect of startups. Or any doc where there’s a high level of entrepreneurship/independent practices (e.g. psych).
- It’s a positive sign if a doc wants to continue to do clinical work at hospitals even if they’re working full time at a company (they wanna keep their clinical skills sharp, that’s good!)
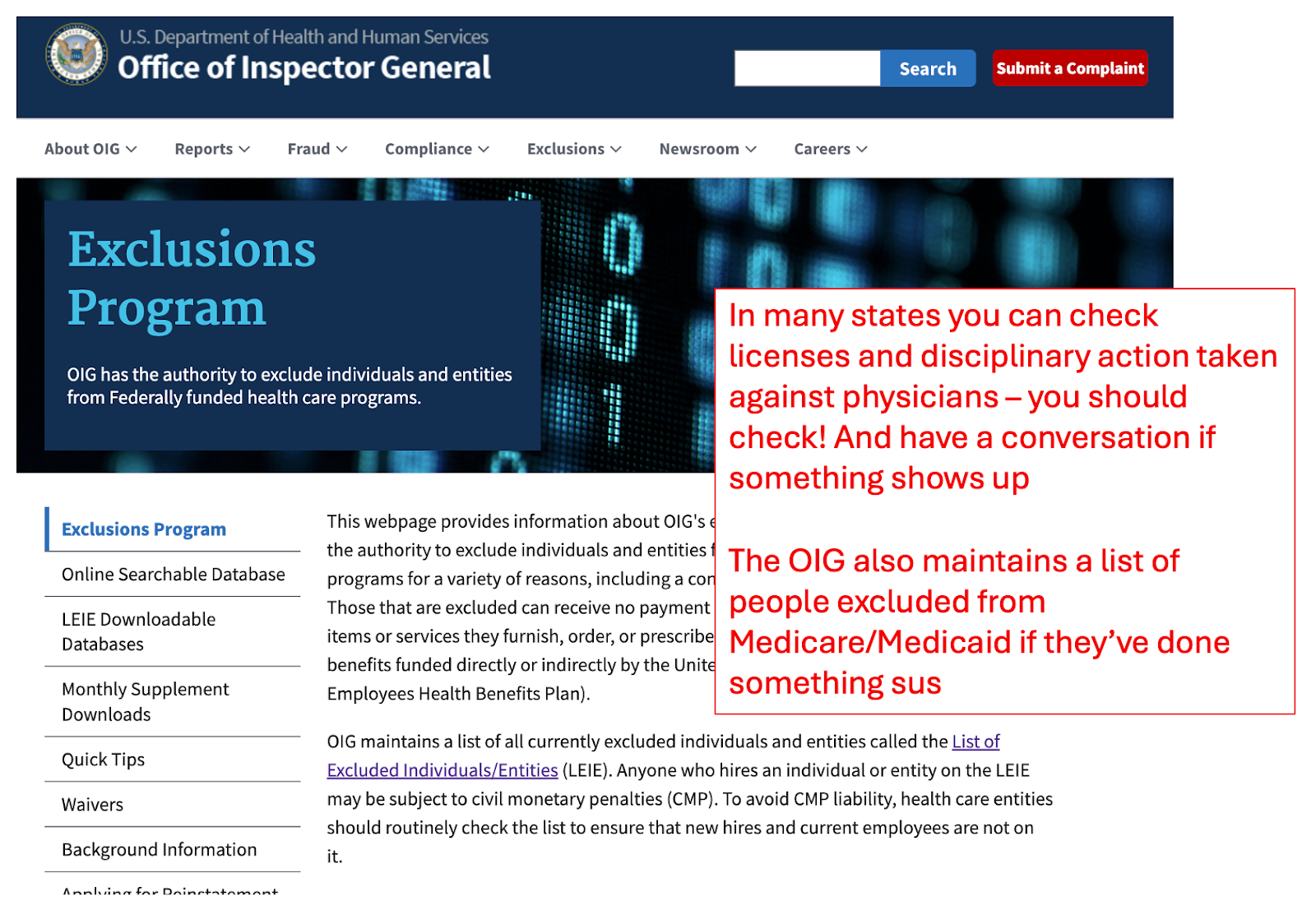
- Please do an actual background check on whoever you choose to hire and see that their license is good to go, where they can and can’t practice, talk through any issues in their record, etc.
- Probably one of the most important skills clinical leaders can have is the ability to communicate. They’re going to have to explain complex concepts to non-healthcare people, teach other clinical team members what the role looks like at the company, etc. This may surprise you but the docs that are well-renowned in their field aren’t always good communicators.
- Like any other leadership, some clinical leaders are good for some stages of companies and not good for others. It’s totally possible that your clinical lead up to Series A is also not the right fit for the company as it scales. Just because you “got a doc” doesn’t mean you’ve checked the box for clinical leadership without mutually re-assessing if it’s a good fit regularly.
- If you need to find clinical leaders, you can use recruiting firms like Oxeon, MDisrupt, etc. It’s a way to fast track finding a person with the skills you’re looking for, but you pay a cost to do so. Alternatively you can search yourself, but then you’re either going to be spending time on vetting in the interview process or coaching someone up to the level you want them to be.
- Honestly I wish more doctors would just start companies themselves, but there’s still a bunch of risk aversion for a whole host of reasons (debt, opportunity cost of time, etc.). If you’re a doc don’t be afraid of starting a company yourself! It’s possible, even a doofus like me managed to do it.
I’m curious to hear what you all think! So reply back with any thoughts on the post, or hot takes on the topic. When you think you need a clinical leader? How do you think clinical leaders should be chosen/vetted/set up for success? Any stories about when it did or didn’t work out. I’ll keep you anonymous if you want.
I’ll post my favorite responses next week.
Thinkboi out,
Nikhil aka. “I can handle the business side”
Thanks to Cyrus Attia and Ajay Haryani for reading drafts of this. We fought, we cried, and they gave very good feedback and pushback.
Twitter: @nikillinit
IG: @outofpockethealth
Other posts: outofpocket.health/posts
{{sub-form}}
If you’re enjoying the newsletter, do me a solid and shoot this over to a friend or healthcare slack channel and tell them to sign up. The line between unemployment and founder of a startup is traction and whether your parents believe you have a job.
Interlude - Apply to Ship It! And Healthcare 101!
See All Courses →Don’t forget the application for our SHIP IT, our healthcare software engineering conference IS LIVE.
If you write or deeply work with code, have some experience working in healthcare, and want to has out how everyone is building things…you should apply to this. It’s small, intimate, and you’ll learn a lot.

And if you feel like you really need to get up to speed on how healthcare works, then you should let me teach you at Healthcare 101 starting 7/13!
This is for anyone hiring teams of non-healthcare people that need to get up to speed quickly (in 2 weeks) - we do group discounts too hit up ya boy. You’ll even learn how to make memes.

Get Out-Of-Pocket in your email


