




Some more thoughts on telemedicine
Get Out-Of-Pocket in your email
Looking to hire the best talent in healthcare? Check out the OOP Talent Collective - where vetted candidates are looking for their next gig. Learn more here or check it out yourself.
 Hire from the Out-Of-Pocket talent collective
Hire from the Out-Of-Pocket talent collectiveHealthcare 101 Crash Course
%2520(1).gif)
Featured Jobs
Finance Associate - Spark Advisors
- Spark Advisors helps seniors enroll in Medicare and understand their benefits by monitoring coverage, figuring out the right benefits, and deal with insurance issues. They're hiring a finance associate.
- firsthand is building technology and services to dramatically change the lives of those with serious mental illness who have fallen through the gaps in the safety net. They are hiring a data engineer to build first of its kind infrastructure to empower their peer-led care team.
- J2 Health brings together best in class data and purpose built software to enable healthcare organizations to optimize provider network performance. They're hiring a data scientist.
Looking for a job in health tech? Check out the other awesome healthcare jobs on the job board + give your preferences to get alerted to new postings.
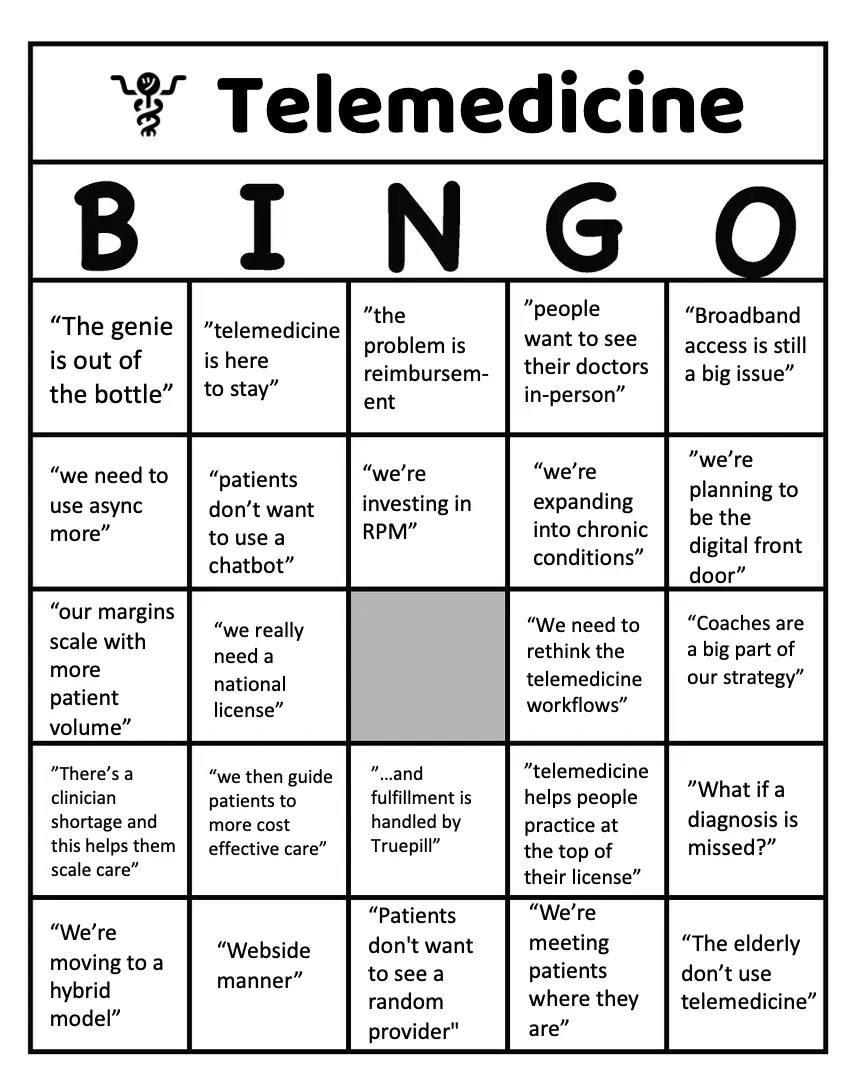
Previously I wrote a post with some thoughts on the current state of affairs in telemedicine. People had lots of great additions to the bingo board to be added in a future edition.
I also asked for your opinions on telemedicine. I got lots of great ones, and whittled it down to a few.
Telemedicine and the trainer/trainee relationship
"I also wanted to offer a different angle to your telemedicine conundrum, which relates to medical/resident training and the future of our doctors -
A big part of medicine is apprenticeship - medical school training, resident training.. In medical school, we often joked 'monkey see, monkey do'. In the US alone, there were 144,660 residents in 2021 out of just over one million active physicians. That's over 13% and there is no doubt that ALL attending physicians were once residents. It is already established that more telemedicine training should be part of medical training (see here and here), but what does telemedicine mean for learning opportunities that require close observation or senior support? One of my good friends, a cardiology resident and pregnant, recently started to work from home as part of a COVID-19 measure to move clinicians home from week 30+ of pregnancy. Although her hospital was well-established in telemedicine, she found it frustratingly difficult to get hold of an attending for questions she had about difficult cases. In a physical clinic, she would have just left her patient in the waiting room, waited for her attending to finish off with their patient (probably in the next room), popped in to discuss the case, and then gone back to her patient. In her current situation, she found it difficult to get hold of the attending or to show them ECG charts.
Telemedicine companies need to keep this in mind and make it available for trainees and trainers to communicate in the absence of the patient - perhaps through a different channel or messaging medium. Logistical tools also need to be available to medical students, not only to observe consultations but to discuss cases with their trainers between appointments. Similarly, while telemedicine creates a tempting tunnel-workflow where clinicians are less likely to be disturbed than in their conventional clinic setting, trainers need to make themselves more available to their trainees for support. There needs to be a fundamental change in healthcare culture where trainers are openly available to trainees rather than trainees having to lose a limb to speak to their trainers. Indeed, telemedicine is in its 'awkward teenage years' and while clinicians try to fit it into the existing healthcare system, we need to ensure that our future generation of senior doctors is not being left behind."
- Dr. April Chan, Medical Content Manager at Medcase
[Nikhil note: One of the things I think remote companies struggle with generally is the benefits that come with random 5 minute “drive by” meetings + colleagues from each other through the osmosis of being in the same room. It’s not surprising to me that those same problems would extend to physicians collaborating with their colleagues.]

Who’s stopping the national license?
"Telemedicine is blocked by licensure, full stop. (scratch your bingo card)
The financials to cover all 50 states (a must have to do telehealth first successfully, otherwise your service is useless the second someone leaves their state) are a nightmare. It can take a year and $2-3K per state to get a clinician covered, and if they leave, their licenses leave with them. And the work is on the clinician. You can't do it for them. State boards lose fingerprint cards, get caught up in scandals delaying approvals, and a dozen other things.
Everyone knows it's bad. Every system hates how licensing works. Every clinician hates it.
Yet no one seems to know why we don't have a national license. Everyone seems to want it. The ATA is massive, and there have been open letters signed by every company and org in the states advocating for relaxing of these laws. Even the Federation of State Medical Boards seems to be pushing the compact.
I cannot figure out who is fighting this! It's like a strawman come to life.We seem to keep writing "let's keep telemedicine" articles addressed to no one. It's as if everyone in healthcare is looking around at everyone else being like "well, are you the one who can fix this?"
Do you know? Do you have any idea who is actually blocking this stuff?"
-Kyle Munkittrick
[Nikhil note: My guess is that it’s a combination of state licensing boards that make quite a bit of revenue from each physician needing to go through it + providers/physicians in a given state that don’t want to introduce more competition within their state]

{{interlude 3}}
McKinsey data is sus
“I think the McKinsey data on physicians hating telemedicine is suspect - having interviewed i'm guessing 500+ physicians (maybe more) in the last 2 years. Physicians are legit the last highly paid profession to not be able to work from home historically and COVID is allowing them to flex their schedules to do all telemedicine or hybrid. So many physicians do not want to be tied to a physical place 6 days a week and having to schedule their vacations a year in advance."
-Stuart Blitz, COO at Hone Health
[Nikhil note: Planning trips with any physician friends basically requires a doodle that encompasses every single weekend of a given year just to find one that works
Touch it, bring it, pay it, watch it, turn it, leave it, stop, format it
“My own opinion is that the pendulum swung way too hard in the direction of telemedicine with an overcorrection caused by the pandemic and unbridled enthusiasm that was never going to be sustainable in a post-pandemic (or at least endemic) world. Sure, telehealth/medicine was underutilized prior to the pandemic, but many mistook the huge uptick in its utilization early in the pandemic as a sign that both doctors and patients were ready to embrace the technology and there was no going back. Never move all of your chips onto the table during a Black Swan event.
Our own experience was that telehealth was better than nothing at all, and it was great that the governor of Massachusetts ordered insurance companies to reimburse these visits at the same level as in person visits. But that was never going to be sustainable either. The process of seeing patients via telehealth was never smooth for a variety of reasons. Technical difficulties, less tech savvy patients (and docs) struggling, convoluted workflows (for Ortho this often meant three screens – one for telehealth, one to review x-rays, and one logged into the EMR), lack of ability to perform a physical exam, etc. In many cases, patients preferred a simple phone call over a video visit. While it was kinda cool to see patients in their own environment and somewhat flipped the script on the doctor visit, it was hard to argue that video added a lot in many circumstances. When in person visits returned and whispers of reimbursement returning to pre-COVID levels, telehealth didn’t stand a chance. It is very difficult to balance in person and telehealth visits in the same day and hard to argue for an entire day or even half day of telehealth only visits.
In Ortho, there are some situations where telehealth might make sense. Certain postop follow up visits, a check-in to see how a patient has responded to an injection or physical therapy a few weeks later, or a check-in for a simple problem. However, it could easily be argued in these cases that a simple phone call is sufficient (if any follow up is needed at all). In fact, this is an area where asynchronous check-ins might make more sense from a work flow and patient/provider convenience standpoint. Hospitals charging facility fees for telehealth is the height of headshaking healthcare absurdity.
Telehealth has a place in the future but not as a retrofit solution that everyone flocked to out of necessity. In order to make it work, the proper processes have to be put in place and thoughtfully integrated rather than adopted out of necessity then abandoned because they were set up to fail. Remote physical exam tools will improve over time, but will it ever be as good or better than in-person for most things? While limited studies seem to indicate it’s the doctors who are resistant to telehealth, I think patients’ desire for this option has been oversold. Will be curious to see what the numbers look like 6-12 months from now. ”
-Benjamin Schwartz, MD
[Nikhil note: At what point do we start teaching telemedicine-first workflows within specialties in med school? I wonder if this ends up being a generational shift in mindset.
Simultaneously, I wonder how much of patients wanting to come in for a visit has to do with their frustration with the current telemedicine tooling - how many people love Zoom in general? How do we make patients feel like they got holistic care over telemedicine, or is that possible?]
Telemedicine is the antidote to $$ going to procedure-driven specialties
“Good post - love the Bingo card! I have very complicated thoughts on this topic, especially since I work for a telemedicine company. One interesting observation I've made that you didn't cover is something I've observed through the experience of my wife, a physician at a large health system. She was frequently spending time calling patients (on her dime) or forcing patients to travel in for a short visit (so she can bill) to review lab results. She's an endocrinologist, lots of labs. Now she can do a quick telemedicine appointment which is way better for patients but also gives her something to bill for in a speciality that generates far less revenue than most. And yes, this is another reason why value based care is far better than fee for service.”
-Anonymous
[Nikhil note: Telemedicine to increase patient touchpoints + revenue as a countervailing force against specialties that derive more revenue from procedures is an interesting dynamic.
Also with gas at an all time high, think about how much indirect cost is actually passed to the patient when we force them to come into the office for visits that could easily be done through the phone]
Thinkboi out,
Nikhil aka. “can I still get a lollipop after a telemedicine visit? the real unsolved problem"
Twitter: @nikillinit
Other posts: outofpocket.health/posts
{{sub-form}}
---
If you’re enjoying the newsletter, do me a solid and shoot this over to a friend or healthcare slack channel and tell them to sign up. The line between unemployment and founder of a startup is traction and whether your parents believe you have a job.
Interlude - Apply to Knowledgefest! And healthcare 101 starts next week!
See All Courses →Don’t forget the application for our Knowledgefest, our healthcare software engineering conference IS LIVE.
If you work in healthcare ops, you want to be here. This is where you learn playbooks, see what other ops people are doing, and build your network. It’s year 5 and we sell out every year - applications are due end of month.
And if you feel like you really need to get up to speed on how healthcare works, then you should let me teach you at Healthcare 101starting next week!This is for anyone hiring teams of non-healthcare people that need to get up to speed quickly (in 2 weeks) - we do group discounts too hit up ya boy. You’ll even learn how to make memes.
.png)
Get Out-Of-Pocket in your email


