




It’s Time For Physician Independence
Get Out-Of-Pocket in your email
Looking to hire the best talent in healthcare? Check out the OOP Talent Collective - where vetted candidates are looking for their next gig. Learn more here or check it out yourself.
 Hire from the Out-Of-Pocket talent collective
Hire from the Out-Of-Pocket talent collectiveHealthcare 101 Crash Course
%2520(1).gif)
Featured Jobs
Finance Associate - Spark Advisors
- Spark Advisors helps seniors enroll in Medicare and understand their benefits by monitoring coverage, figuring out the right benefits, and deal with insurance issues. They're hiring a finance associate.
- firsthand is building technology and services to dramatically change the lives of those with serious mental illness who have fallen through the gaps in the safety net. They are hiring a data engineer to build first of its kind infrastructure to empower their peer-led care team.
- J2 Health brings together best in class data and purpose built software to enable healthcare organizations to optimize provider network performance. They're hiring a data scientist.
Looking for a job in health tech? Check out the other awesome healthcare jobs on the job board + give your preferences to get alerted to new postings.
Recently, I hosted a discussion/gave a presentation about how we can get to physician independence.
Below is a summary of my report and the discussion. You can get the full slides and recording here.
The decline of the private practice
Imagine you’re in ancient times, 8 AK (after Krishnan) in the early 2000s. People had designated primary care physicians, health insurance premiums weren’t wylin’, and MTV still had dating shows that made absolutely 0 sense and probably cancellable like “Date My Mom”. During this era, about 70+% of practices were owned by physicians.
But all that started changing. It’s hard to pinpoint one specific thing that shifted, but my understanding is that it was a combination of small things that led to private practices declining (feel free to let me know if I’m wrong):
- Reimbursement from government programs like Medicare/Medicaid were not growing as quickly. Commercial insurance rates were different. These rates could be negotiated higher if the hospitals increased their sizes and had tighter controls over referrals. This led to hospitals scooping up lots of smaller groups and practices.
- There was a big push for decreasing medical errors and adopting electronic health records, which increased the administrative overhead of practices.
- The administrative needs to handle the increasing rules that payers were imposing began getting more complex.
- The amount of medical debt for graduates rose substantially to an average of ~$216K+. This makes a stable salaried job more appealing and yields boomer-y diatribe like:
“When I was young, you didn’t blink an eye at being on call all the time, going to the hospital, being up all night,” said Dr. Gordon Hughes, chairman of the board of trustees for the Indiana State Medical Association. “But the young people coming out of training now don’t want to do much call and don’t want the risk of buying into a practice, but they still want a good lifestyle and a big salary. You can’t have it both ways.”
- Because of the above, practice owners who normally might consider selling practices to younger physicians in a succession plan were now uncertain whether they’d be able to do that. So when a buyer like a large hospital or PE group comes knocking with some cash, it becomes increasingly tempting to sell.

As a result, we’ve seen the decline of private practice and the rise of hospitals as the employer of choice for physicians. In fact, only a few years ago did we see the definitive switch where more physicians were employees of corporations than physician-owned groups.

Why does physician independence matter?
We should want more independent physicians for a few reasons.
1) Hospital services are the most expensive part of US healthcare and continue to increase prices much faster than physician services and clinics. A big part of this is the monopolistic pricing power that hospitals now have since they’re so consolidated. In many cases, the larger hospital system will extend the “privileges” they have to all of the practices they acquire (e.g. name brand recognition, non-profit status, multipliers for services they give, etc.) in ways that can mislead patients or cost the system more money. On top of that, having much larger hospitals that are a Frankenstein abomination of many different care settings and services means you need way more admin to be able to coordinate everything internally, which increases spending there as well.
With more independent physicians, we could see more competition in care delivery, which should slow price growth.

And despite the higher prices, that revenue doesn’t seem to be going to physicians. If you look at revenue generated by different specialties vs. how much those physicians earn, the growth is…not equivalent. Though I wouldn’t say doctors are exactly going hungry, they’re probably shopping at Whole Foods, not Erewhon.

2) But it’s not just prices that are going up; it doesn’t seem like quality is actually improving, which was part of the reason why hospital consolidation was encouraged. This study looked at many integrated delivery networks and found as they took up more of the market, their quality didn’t improve. Other studies looked at hospitals immediately post-merger/acquisition and found many of their quality metrics went down. The quality of waiting rooms has increased, which is not something I should know.
And with hospitals being stuck in a fee-for-service paradigm without much of their revenue tied to risk, they don’t really push to improve quality metrics. In fact, for Accountable Care Organizations, there’s been more success in physician groups than hospitals nowadays.

3) Ownership and burnout are intertwined. We’re experiencing an epidemic of burnout for frontline staff and clinicians. I think a big part of this is that physicians don’t feel control over their schedules, the tasks they’re given, the tools they use, or financial upside from the extra work they’re asked to do. Small practices and clinician owned practices seem to be less likely to have high burnout rates.
Even outside of healthcare, I think a lot of people who’ve started a company or left a full-time job to consult will tell you that they work much more but feel less burnout because they’re choosing their work and feel a more direct correlation between the work they put in and the money they make. I can tell you personally from starting a business that despite decaying on a physical level, finding gray hairs…everywhere, and becoming completely desensitized to cortisol, I am very fulfilled and happy.

4) I think we’d see more innovation in care delivery if we have more small and medium size practices. Practices could build more natively to a payment system that makes sense for them and focus on it. A practice that takes only cash, or only sees the elderly, or maybe just focuses on a specific disease area will be purpose built to serve those specific populations. In other industries, this kind of segmentation of customers allows companies to build in the most cost-effective way to serve the specific end customer they’re targeting. In healthcare, large hospitals build to serve everyone, and as a result, spend a ton on operating and capital expenses which they then need to recoup.
That innovation also extends to the tooling side. Smaller practices are more likely to try out point solutions that solve a specific pain point. For digital health companies, these are shorter sales cycles, less brutal integrations, and it allows them to compete on user experience since the practice owner is usually the buyer and user. This leads to quicker product iterations and the ability to be more capital efficient since you’re actually making money earlier.
---
But even though there seem to be these benefits from physician independence, we’ve been seeing more consolidation over the last 10 years. This seems to be only getting worse.
…or is it????
The inflection point for consolidation
A part of me thinks (or maybe just hopes) that we might be at an inflection point to potentially reverse the rampant hospital consolidation that’s been happening and instead make it easier for physicians to strike out on their own. There are a few reasons why.
It’s possible that hospitals are losing their appeal as a place of employment given all the ways they treated staff during COVID. Turns out banging pots and pans, wellness webinars, and “healthcare workers are heroes” signs aren’t enough to offset the massive divide felt between the people in the clinics during COVID and the people giving them orders from afar.
Looking at a survey of graduating residents and seeing where they want to work, the interest in working at a hospital has flattened for the first time. Increasingly more residents are unsure of what they want to do, which either means there’s an opportunity to build something new and appealing for them, or they don’t want to practice at all, which is…bad. Like, societally.

Beyond their appeal, hospitals are also losing their leverage. Usually this is when I point to some FTC mention where they vaguely say “oh ho ho hospital consolidation is bad” and that antitrust scrutiny is going to increase. But I think both of us know…we probably shouldn’t bet on this.
Instead I think it’s the No Surprises Act which is the driving force here. Thanks to this act, hospitals can’t push out-of-network bills onto patients, and instead will take the median in-network reimbursement for the service in that geography (called the QPA). Therefore, the negotiating now starts at QPA for insurers, and can’t REALLY move too far away from that. Here’s a thread where someone shows how Cigna is refusing to budge on rates using the No Surprises Act as a justification.
Historically, insurers have had to walk a fine line with not pissing off any major health systems since they’ve needed them in-network. Imagine being in Cleveland and being in an insurance plan without the Cleveland Clinic, you’re basically asking to get bullied and laughed at. But now with more negotiating leverage, payers can actually lean into supporting more independent practices and maybe even helping them get started. I’ve always wondered why insurers didn’t try harder to support a more thriving independent physician ecosystem since that competition should work in their favor. My guess is that the big hospitals exerted some pressure to prevent that. Maybe now, payers can be more active in helping physicians become independent.
Not only does it help loosen the stranglehold hospitals have, the No Surprises Act theoretically allows small practices to get paid UP to the QPA, which they might not have been able to negotiate before. Getting enough reimbursement from payers has been a worry for independents, and maybe the No Surprises Act makes that less of an issue.
While hospitals were losing their leverage, individual physicians were accumulating theirs. The shortage of physicians combined with the surge in healthcare demand has yielded insane signing bonuses to get physicians to join (up to $400K!!!). As the physician shortage is projected to get worse, individual physicians have more leverage.
On top of that, individual physicians are more trusted than the organizations they work for. Combine that with new tools that allow physicians to connect directly with their patients like social media, and you start to see individual physicians with their own “followings” who can potentially turn them into patient acquisition channels for their own practices. We’ve already talked about the rise of the physician creator previously, so I won’t rehash that.

The final nail…opening the coffin I guess? Since physician independence has been dead? (Whatever, not important).
The final nail is the tools that have made it easier for physicians to start practices. For example, a physician can start a telemedicine-first practice for $50-100/mo instead of needing tens of thousands of dollars and constraining to a specific geography. You can start a telemedicine practice, build a patient panel through online marketing or e-consults/second opinions, and eventually build a large enough panel to support a hybrid in-person/online practice.
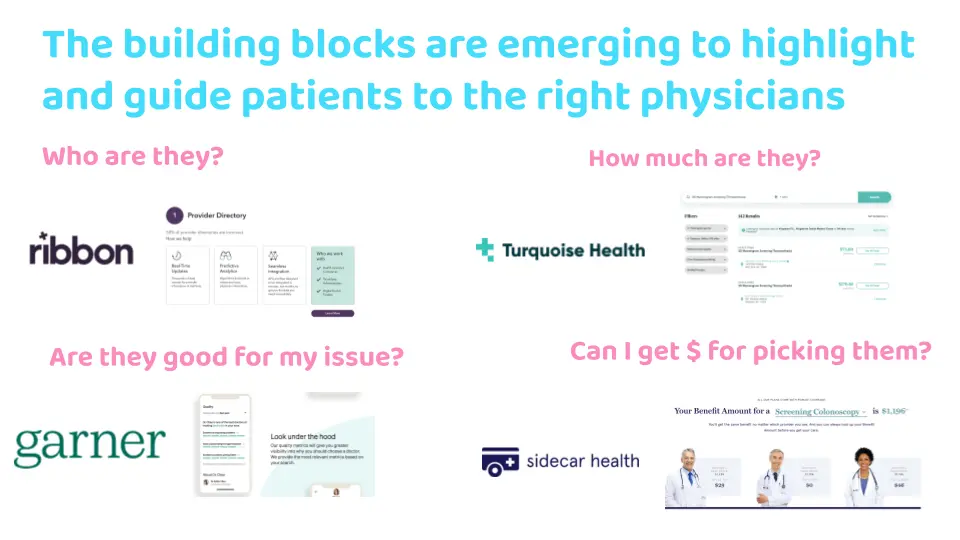
And the tools to actually guide patients to those doctors are emerging. Like figuring out who the doctor is, if it’s the right doctor for them, what they charge, and creating financial incentives for patients picking them if they’re cost-effective. When these powers combine, they form Captain Plan-it! (a visit to the doctor).
I still think there are even more opportunities to enable this transition. If you look at some of the reasons that physicians LIKE to be employed, maybe there are ways to tackle those and make it more palatable for them to be independent. I talk about some other companies tackling these opportunities in the presentation itself, so you can see them in the full deck.

{{interlude 3}}
Conclusion and other notes from the discussion
It’s pretty clear that the current trajectory of hospital and PE buying physicians isn’t sustainable. I think there’s reason to bet that we’re at the inflection point. And to be clear, I don’t think everyone is going to become independent, but the choice between running your own practice and working for a corporation should be less heavily weighted towards corporations.
In the deck, I talk about the interesting case of Tryon Medical Partners. A group of physicians managed to secede, sued to get out of their non-competes with a major health system, start their own practice, and take their patients with them. It highlights how it might actually be easier for groups of physicians to go independent, pool money, and have better control over their referral pathways vs. doing it solo.
Maybe this is the canary in the coal mine for physician independence. In fact the Executive Order signed last year which aimed to ban/limit non-competes, with physicians being specifically talked about. Anecdotally some senior physicians have mentioned non-competes as a big reason for not starting their own practice, so maybe this is one less barrier to stop them and Tryon is an example of success on the other side.

I had a great discussion with the panelists as well about the topic of independence, with each of them bringing very different perspectives. We had:
- Mario Amaro, MD - Founder/CEO of Ease
- Lisa Lucas, DO - Direct Primary Care (DPC) owner + DPC Medical Director of Taro Health
- Michael Cui, MD - Rush University Medical Center
- Benjamin Schwartz, MD - Community Orthopedic Surgeon
You should listen to the whole discussion, but some particularly interesting points that came up (not all of these are my opinions, just things that came up):
- For physicians that want to work in a value-based care model, it’s really hard to do that independently. If you have a small number of patients and are on the hook for their total cost of care, a few sick ones can nearly bankrupt you. Maybe there’s an opportunity to create stop-loss insurance or captives for groups of independent physicians in value-based care models? For practices that are successful in other value-based care models, they can become the victims of their own success if they show they can deliver care for cheaper since they would get reimbursed less in future years (but have already invested in upfront infrastructure and staff to be a part of the value-based program).
- Coordination between physicians that aren’t part of a hospital is still a challenge. How do you get referrals if you’re a specialist going independent? If you’re a primary care doc referring to a specialist, how do you make sure both groups keep their records updated about the patient’s status? DPC docs have more time per patient, so they spend some of it chasing down information and coordinating with specialists.
- The flip side is that coordination amongst physicians going independent together is new territory. When education on how to start a practice is a barrier, doing so with other physicians going through the same process is helpful. Ease has fellowships and cohorts for people looking to start a practice and direct primary care communities share a lot of best practices with each other.
- Finances are a barrier. On the personal finance side, getting access to loans, having high amounts of debt, and physicians generally starting careers when they’re older with families/other expenses are all factors that make it difficult to get started. Maybe the rise of physician gig work can help offset that income loss a bit. Plus, once a practice starts growing, there’s a cash flow crunch issue because of the lag in insurance reimbursement + unpredictability of it’ll get approved once the “types” of visits you do expands.
- My flowery shirt looks cute on camera but my forehead is shiny.

- How much should doctors know about the business of healthcare vs. the ever expanding amount of literature in their field? It’s easy for doctors to just say “the business is someone else’s problem, I just do medicine”. Doctors should probably know how this impacts care at the very least (e.g. if a patient can’t afford their copay, they’re going to be non-compliant). Knowing the expected costs and revenue of a practice may make it seem more accessible to start one. Right now because training is so focused in academic settings, there can be way less exposure to the workings of private practice.
There was lots of other stuff on startup costs of direct primary care, challenges as practices grow, and the role of insurance in enabling or preventing independent physicians from starting. We also talked about what Taro Health is, what Ease does, getting your practice bought, and what it’s like to create a new clinic within a health system.
Check out the full deck and talk. There’s a lot of opportunity here, and I think more companies should be working on this since it’s a meaningful problem.
Thinkboi out,
Nikhil aka. "I-N-D-E-P-E-N-D-E-N-T yeah you know what that meansss"
Twitter: @nikillinit
Other posts: outofpocket.health/posts
Thanks To Dan O'Neill and Afnan Tariq for looking at drafts of this
{{sub-form}}
---
If you’re enjoying the newsletter, do me a solid and shoot this over to a friend or healthcare slack channel and tell them to sign up. The line between unemployment and founder of a startup is traction and whether your parents believe you have a job.
Interlude - Apply to Knowledgefest! And healthcare 101 starts next week!
See All Courses →Don’t forget the application for our Knowledgefest, our healthcare software engineering conference IS LIVE.
If you work in healthcare ops, you want to be here. This is where you learn playbooks, see what other ops people are doing, and build your network. It’s year 5 and we sell out every year - applications are due end of month.
And if you feel like you really need to get up to speed on how healthcare works, then you should let me teach you at Healthcare 101starting next week!This is for anyone hiring teams of non-healthcare people that need to get up to speed quickly (in 2 weeks) - we do group discounts too hit up ya boy. You’ll even learn how to make memes.
.png)
Get Out-Of-Pocket in your email


