




Answers: How Much Info Should A Patient Get?
Get Out-Of-Pocket in your email
Looking to hire the best talent in healthcare? Check out the OOP Talent Collective - where vetted candidates are looking for their next gig. Learn more here or check it out yourself.
 Hire from the Out-Of-Pocket talent collective
Hire from the Out-Of-Pocket talent collectiveFHIR 101

Featured Jobs
Finance Associate - Spark Advisors
- Spark Advisors helps seniors enroll in Medicare and understand their benefits by monitoring coverage, figuring out the right benefits, and deal with insurance issues. They're hiring a finance associate.
- firsthand is building technology and services to dramatically change the lives of those with serious mental illness who have fallen through the gaps in the safety net. They are hiring a data engineer to build first of its kind infrastructure to empower their peer-led care team.
- J2 Health brings together best in class data and purpose built software to enable healthcare organizations to optimize provider network performance. They're hiring a data scientist.
Looking for a job in health tech? Check out the other awesome healthcare jobs on the job board + give your preferences to get alerted to new postings.
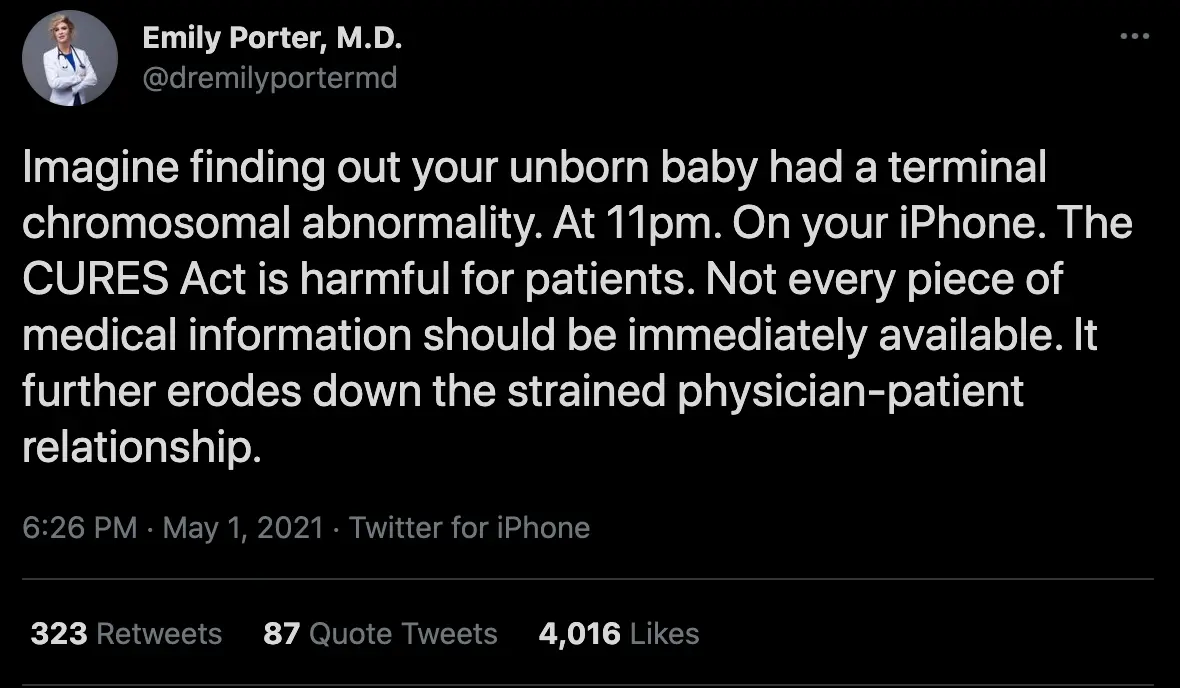
On the last episode of “Out-Of-Pocket gets people mad”, I gave my thoughts on whether patients should have access to their data immediately or not (thanks to the 21st Century Cures Act which enables this). It was inspired by this tweet.
This week, I’m posting some of my favorite responses. I got so many good ones that I included 5 (but about 60 of you mailed in, all of them were very thoughtful).
The split was pretty even, with clinicians arguing the data needs context (and googling around will ignore the patient-specific context) and patients arguing the timeliness of data is important and physicians shouldn't make that choice for them. Other interesting ideas that came up
- Physicians should need to prove that NOT giving the data is actually beneficial. Just because it's status quo currently doesn't mean the default shouldn't be challenged.
- Patients should be able to choose the level of interpretation they want, similar to when you make robo-advisor choices
- Releasing the notes as they are will cause chaos, but over time either the notes will get more readable or middle layers will emerge that converts the notes into readable forms for patients (either software will do this or non-physician interpreters e.g. how genetic counseling is a separate area nowadays)
*no answers represent the employer that these people work for, and other disclaimers
---
Have you considered your marriage is the problem?
“I strongly believe patients should have access to all of their data. My wife has a chronic autoimmune condition and has seen dozens of GPs and specialists over the past decade. I go to most appointments with her, and my experience with about 50 doctors across multiple highly regarded medical systems is that perhaps 10% are fantastic, 40% are ok but not especially helpful ("thanks for telling me about your symptoms today, not sure what this could be, please see another specialist"), and 50% are somewhere between poor and awful (dismissiveness, gaslighting, saying "maybe it's anxiety or a bad marriage" instead of evaluating demonstrable symptoms, refusing medical testing and treatments, ...).

As a result of these interactions, my wife and I have only made progress on her illness and treatments by doing our own research and advocating for treatments and tests with the 10% of doctors that are empathetic and trying to help however they can. It's through this self-advocacy that we figured out potential underlying causes of her condition, which drugs might work, etc. The more data we've had, the more research we've been able to do and the more progress we've been able to make.
To me, keeping health data away from the patients themselves is deeply unethical. It's a paternalistic nanny state mentality that suggests patients are dumb and doctors are incredible, when in fact the opposite is often true. Furthermore, perhaps if notes like "difficult patient" or "I think it's anxiety and not a real medical issue" were visible to patients, then doctors would have a higher bar for writing them and would be less dismissive of actual symptoms. For example my wife has a documented history of dangerously low blood levels of a key electrolyte, as well as documented instances of severe orthostatic tachycardia. And yet, on an ER trip a few years ago, a doctor didn't want to order labs for the electrolyte because they didn't believe my wife had issues with it, and they forced her to stand up from a wheelchair to demonstrate that she had an orthostatic condition and wasn't just faking it. It's infuriating that this doctor 1) can do that, 2) can then make a note that my wife is a difficult patient for pushing back on his dismissive anxiety diagnosis, and 3) whatever notes they write aren't shared with us but do influence the opinion and disposition of any future doctor that reads them.
It's not hyperbole to say that keeping data from a severely ill patient who has the ability to research and improve their condition can be equivalent to murder in extreme cases. We give people agency over their health by letting them diet and exercise however they want, and we should increase that agency by making their patient data more accessible, too.”
-Anonymous
How much is relevant for you?
“I think a lot of people on Twitter forget how low health literacy can be among patients. For example, patients who aren’t savvy enough to use Twitter and reply to such a thread …
A lot of what is written in radiology and pathology reports is meant for the clinician. When the radiologist says “chronic ischemic changes”, that is a natural finding that can be seen with age - but patients who Google it may think they’ve had a stroke. When it says “most likely infectious or inflammatory, cannot rule out malignancy,” that is the radiologist covering their own bases and not an indication that anyone believes there is cancer there.
So much of medicine is based on context. There is a reason physicians go through medical school, residency, and often fellowship, before they see patients on their own. It’s not possible for patients to replace this knowledge base and experience by googling a couple of words they see in the chart.
Patients have started calling in to physician offices, demanding to move appointments up by as little as 24 hours because they are so anxious about what they’ve read in the radiology report. They come into the office having highlighted parts of their medical record, asking why they were never told certain things that have no clinical significance and have no impact on their health. Some patients fixate on these meaningless abnormalities and feel as though their physician isn’t telling them the truth when something is wrong.
Physicians are already pressed for time in our current healthcare system, and now much of that time is being dedicated to alleviating anxiety that didn’t need to exist in the first place. This leaves less time for crucial history taking and counseling that would otherwise be done during that visit and would likely be more productive for the patient.
I agree that patients should have access to their information and their records, but I disagree that this access should be granted instantaneously, before a discussion with the physician can take place. Patient-facing physicians exist for a reason. It is critical for them to act as an honest broker of relevant information to the patient, to explain the pertinent information, to engage the patient in decision-making, and to offer options that make sense in context. Giving patients raw information without these considerations and a safe space to immediately ask questions and plan next steps seems likely to do more harm than good.”
-Anonymous
Interpreting data to the right level of literacy
“Great post. I'm an ER doc, and while I'm unambiguously happy with the progress towards more transparency---as opposed to a 1950s-style chart diagnosis of say 'hysteria' and the like---I think a few caveats are worth mentioning.
My job is to diagnose and treat diseases. Thankfully that involves translating what I'm doing to someone's body in terms they understand. I like that. It empowers my patients when they comprehend what's happening. And honestly, I tailor it to my audience. A 16 year-old and an rocket engineer and a mom who's cared for her son's cystic fibrosis for 20 years all have different levels of health literacy, and it's up to me to meet them there. The sticking point is: sometimes the direct (and more importantly immediate) access to that information gets in the way of that meeting, rather than facilitate it.

Last week for example, a young parent became deeply anxious when they found out their child had coronavirus via the patient portal just minutes before I could tell them. It wasn't Covid-19, but a mostly harmless, pre-pandemic version of a virus that causes the common cold. I have to ask: what is the virtue in them finding out this test result and experiencing the panic they felt without a physician's reassuring translation of it? (To any early objectors, the result actually read 'not covid-19' parenthetically, but the understandable anxiety had already done its damage). Another time I had to field questions about a different patient's finding (again via the web portal) his mean platelet volume was 1 point above assay (a clinically irrelevant finding in this scenario) while trying to bring the conversation back to some other, way more important results.
Perhaps it's easy to say that it's just part of the job, but why would anyone want to make their doctor's job of reassuring you harder? I'm not trying to slip one by you to score a bigger commission (I'm salaried), but I am trying to not order, or for that part, highlight, results that are, in the proper clinical context, totally benign. If immediate and untranslated results to all test results are to be considered progress, then we ought to be prepared for these inevitable side effects.“
-James Gaylor
{{interlude 3}}
Should providers have turnaround time requirements?
“Unquestionably, 100%, yes — patients should have access to the data as soon as it becomes available. My own personal experience is not nearly as harrowing as the one described in the tweet, but shares a different perspective. In spring of 2019 I was feeling quite off psychologically, so I went to an OBGYN and asked for a hormone panel along with comprehensive bloodwork. When I left the office I was told that “no news is good news” — they assured me that if anything concerning showed up in my labs they would let me know ASAP. Weeks went by without hearing anything from them, which — though anxiety provoking — led me to believe that everything had turned out completely normal.
3 FULL MONTHS after my original appointment I received a call from the office. When I answered, a breathless nurse on the line thanked god for finally being able to reach me, and launched into a ridiculous narrative about how they’d been trying to contact me for “months” about my lab results. It couldn’t have been true — I had no voicemails, no missed calls, no emails, NOTHING from this Dr.’s office. Her tone and general demeanor on the phone call led me to believe something horrible had happened. After all, she’d started the call by telling me we “needed to talk” about my lab results. My heart was racing, I started sweating, I collapsed onto the floor of my apartment waiting for the bad news. She proceeded to tell me I’d tested positive for Hashimoto’s, a disease I’d never heard of. I was terrified (it sounds scary when you don’t know what it actually is) and asked what that meant — she told me she didn’t really know, that I needed to speak with my PCP about it ASAP. Before hanging up, she also casually informed me that I’d tested positive for an STD. Suffice it to say that this phone conversation was a remarkably unprofessional way to deliver this news, especially given the 3 month delay.
I made an appointment with my PCP right away, and asked to be retested on both the Hashimoto’s front and the STD front, as the 3 month delay made me question the validity of the bloodwork. It turned out that my Hashimoto’s result was legit, but the STD had been a false positive. Though I’m relieved that it wasn’t a real test result, to this day I am floored that an OBGYN believed I had an STD and let me go on living my life for 3 full months without letting me know....While I was with my PCP, I asked her what a Hashimoto’s diagnosis meant for me. She tried to answer but struggled with it, and then I watched in disbelief as she pulled up her computer and Googled “Hashimoto’s” in front of me. She proceeded to read me the WebMD page that I’d already read in full after the OBGYN office had called me. She then told me I should probably speak to an endocrinologist, and sent me on my merry way with an extra $400 charge, as my visit had “required medical expertise beyond the expectations for an annual physical.”

I’m realizing that I’ve devolved slightly into bitching about shitty doctors, but the moral of this story is that my experience would have been 1000x better if I’d received those test results right away. The “no news is good news” model does nothing but provoke anxiety, worsen patient experience, and create opportunities for mistakes like the one I experienced. If you are going to receive any form of news, receiving it sooner is always better. With that being said, receiving those test results with zero context was as harmful — if not more harmful — than receiving those results 3 months late. There is no question that the onus is on the physician/medical system as a whole to deliver patient data in a way that is accessible to people who have no medical education. The existence of Dr. Google, Reddit, and pubmed means that any literate patient with internet access will be able to figure out what their data “means”. I found 100 good answers to the question of “what is Hashimoto’s” on the afternoon that the OBGYN called me. I found no trustworthy answers to the question “what does Hashimoto’s mean for me?” You could teach a 5-year-old the reference ranges for the Hashimoto’s test and they’d be able to diagnose it…IMO, the future of what it means to be a doctor is not that you have those ref ranges and diagnoses all memorized (as evidenced by my PCP Googling Hashimoto’s in front of me), but that you can communicate this information to patients in a way that is educational, respectful, and empowers them to make involved, informed decisions. “What now?” is as important -- if not more important -- than “what is it?” and we should strive to create a system where the answers to both of those questions are delivered at the same time.”
-Yasmeen Almog (Twitter, Linkedin)
Covermymeds vs. Covermyass
“I think there are three primary reasons for medical notes. 1. Medical reasoning and communication 2. Billing 3. Legal.
1. Medical reasoning. Regarding medical reasoning, most of the time it does not matter to me whether a patient reads my notes or not. The only times I have a pause is when we are pursuing tests against a patient’s personal wishes: for example if a family member brings in a patient because they think he or she is suicidal but the patient denies suicidal intent. In those cases, we play a balancing act between communicating things to patients and communicating things to the rest of our medical colleagues. This also becomes relevant if we disagree with a patient’s opinion about their disease. This happens for example if a patient believes their symptoms are due to something like chronic Lyme disease but all the evidence goes against that direction. These examples are usually the minority in medicine.
2. Billing. Truth be told, most medical notes and tests are filled with fluff to satisfy billing requirements. When I read notes from other providers, I toggle the ‘manual’ button to omit every word that was from a medical template or copied from a previous record. If there’s something I really want to know, I call my colleagues to get their frank opinion. Half of the notes are garbage. That’s partly why I’m a little down on people parsing medical notes for AI. Doctors document physical exams that they don’t do or review or systems questions that they don’t ask.
3. Legal. A lot of language in medical notes is written in ways to decrease liability. For example, Radiologists often write clinical correlation is recommended and hedge on their impressions.

Back to the original point for whether notes should be shared with patients, most of the time it does not matter. Regarding that original tweet, no pathologist is going to submit their results at 11 pm. Let’s be real.”
-Anonymous
Thinkboi out,
Nikhil aka. “call me, beep me, if you wanna reach me (with my lab results)"
Twitter: @nikillinit
Quick Interlude - NEW COURSE ON FHIR! KNOWLEDGEFEST APPS DUE SOON!
See All Courses →So...what actually is FHIR? I get this question a lot, but there's never really enough time to explain it and also I would just mumble "technical standard" and walk away.
So we decided to do a standalone free FHIR 101 course in partnership with Redox! Over 3 days in August we'll go over the spec itself, how it differs from other healthcare information standards, and practical tips to build with it.
I wanted to call it FHIR fest but it got nixed. You can sign up for it here, it's FREE and it's 8/25-8/27.

And a reminder that Knowledgefest apps are due this week. If you want to be in a room with the best ops people in healthcare, you should apply like TODAY.
We sell this conference out every year - all workshops, learn how people are building and scaling in healthcare, application based so we only take the best. We have people from Commure, Clarity Pediatrics, Pomelo, and Waymark already coming, join the squad.

Get Out-Of-Pocket in your email


