




Scaling Organizations, Patient Payments, and Collections with Lora Rosenblum
Get Out-Of-Pocket in your email
Looking to hire the best talent in healthcare? Check out the OOP Talent Collective - where vetted candidates are looking for their next gig. Learn more here or check it out yourself.
 Hire from the Out-Of-Pocket talent collective
Hire from the Out-Of-Pocket talent collectiveHealthcare 101 Crash Course
%2520(1).gif)
Featured Jobs
Finance Associate - Spark Advisors
- Spark Advisors helps seniors enroll in Medicare and understand their benefits by monitoring coverage, figuring out the right benefits, and deal with insurance issues. They're hiring a finance associate.
- firsthand is building technology and services to dramatically change the lives of those with serious mental illness who have fallen through the gaps in the safety net. They are hiring a data engineer to build first of its kind infrastructure to empower their peer-led care team.
- J2 Health brings together best in class data and purpose built software to enable healthcare organizations to optimize provider network performance. They're hiring a data scientist.
Looking for a job in health tech? Check out the other awesome healthcare jobs on the job board + give your preferences to get alerted to new postings.
Today I’m interviewing Lora Rosenblum, Director of Business Development at Cedar. We talk about various different tree types.

Just kidding, we discuss:
- Scaling customer success teams
- MIPS and whether it’s worthwhile
- Why healthcare bills are so confusing and steps that happen in the backend
- Healthcare ideas she would start
- Helping women of color with salary negotiations
1) What's your background, current role, and the latest cool healthcare project you worked on?
- I'm the Director of Business Development at Cedar. We leverage technology to improve the patient financial experience. In my role, I focus on strategic partnerships, specifically commercial opportunities that grow the business.
- I joined Cedar weeks after (remotely) graduating from an MBA program. Before business school, I spent the majority of my post-college life at growing health tech companies in New York, splitting my time between Oscar and Flatiron. At both companies, I held Operations-focused roles, which is how I learned that I adore building and growing health tech businesses.
- During business school, I co-hosted the Pulse Podcast. I spent a year and a half interviewing people that I admire from across the healthcare space, including: Halle Tecco (Natalist), Dr. Melynda Barnes (Ro), Anmol Madan (Livongo), Lisa Suennen (Manatt), Florian Otto (Cedar), and Mike Botta (Sesame). Having an actual reason to engage with these people and learn about their career paths was a fascinating and rewarding experience. On top of interviewing the best of the best, my co-hosts and I spent a lot of time figuring out how to scale our reach in a short amount of time, which is just the type of thing I love working on.
[NK note: I was never interviewed, but I totally understand]

- Business school is also where I was able to give investing a try, both through Contrary Capital and as a Flare Capital Scholar. These opportunities taught me how to think about building and scaling businesses while providing insight into deal-focused roles. I like to think that my current BD role is a blend of the aspects I enjoyed from investing (creative solutions to business problems and a lot of selling, selling, selling) coupled with a strong operational orientation. I am definitely an operator at heart.
2) At Oscar you helped work on scaling the customer service team. A lot of healthcare services companies get to a point where they need to scale this part of the business up. What were the toughest/most surprising issues you ran into as you built this out and how'd you solve them?
- It's easy for scaling tech companies to overlook how many legacy manual processes they will have to manage - it's impossible to scale everything at once, which leaves a long tail of opportunities that can become urgent really quickly. At Oscar, within the Service org, I oversaw our claims escalation processes thinking about how we could resolve challenges at scale to minimize impact to members. From a process perspective, my role entailed understanding everything from claims submission to nuances of member denials.
- In 2015, we went through an exercise of bringing our outsourced claims processor in-house, and we decided to start with our mailroom capability for the 2016 plan year. We converted a tiny conference room into our new "mailroom", ready to go on January 1, 2016. This was also the year we first entered Texas and California, so providers from these states were learning our claim submission processes. By mid-January or February, once members started seeing their providers for the 2016 plan year, we became inundated with paper claim volumes that far exceeded our projections. There was a lot of risk exposure in letting these claims pile up, primarily financial penalties that we could incur for not processing claims in time (regs which of course differed on a state-by-state basis). I remember staying late with my team, manually stamping received dates on the claims (which, on top of the processing timelines, is also important because providers need to submit claims within a specific window, known as 'timely filing') and physically scanning claims forms to upload into our in-house tracking system. Our scanner sucked and it took forever. Some of the documents were so big (usually medical records for appeals) that they were bound by massive rubber bands. I spent a lot of time with a six sigma certified colleague learning about single process flow and why it was more effective than batch processing. I remember trying to trace these massive paper packets to clearinghouses so that we could encourage providers and their partners to submit electronically. It was unglamorous, but also an important thing to fix!
- I tell this story because it's an important reality to scaling a company! Most people have a hard time acknowledging the unglamorous sides of startup life outside of their organizations. I am all about it.
- I'm also happy to talk about the people side of scaling a CS org....I managed a team of five and learned so much from that!

3) At Flatiron Health, you worked on the MIPS product. How hard is it for physicians to be eligible/participate in MIPS and how does an EMR help there?
- For those unfamiliar with the program, MIPS stands for Merit-Based Incentive Payment System. The program was developed as part of the Medicare Access and CHIP Reauthorization Act (MACRA) of 2015. MIPS essentially consolidated legacy programs that assessed quality (PQRS), cost, and clinicians’ use of technology (Meaningful Use) into a singular program.
- At the start of the program in 2017, it was not hard to be eligible for MIPS. There was a patient volume and/or billings threshold, but it was not (and I believe still is not) super high. Most of our Flatiron providers were eligible, and for those providers not eligible as individuals, you can also participate as a group.
- EMRs are helpful to the extent that they include a lot of the relevant data elements that CMS is looking for during submission. The difficult part comes when you're trying to extract and submit these pieces of data. There are specific ways in which CMS is willing to accept data (which includes EMRs), but this means that providers are at the mercy of how their EMR intends to make the data available for submission.
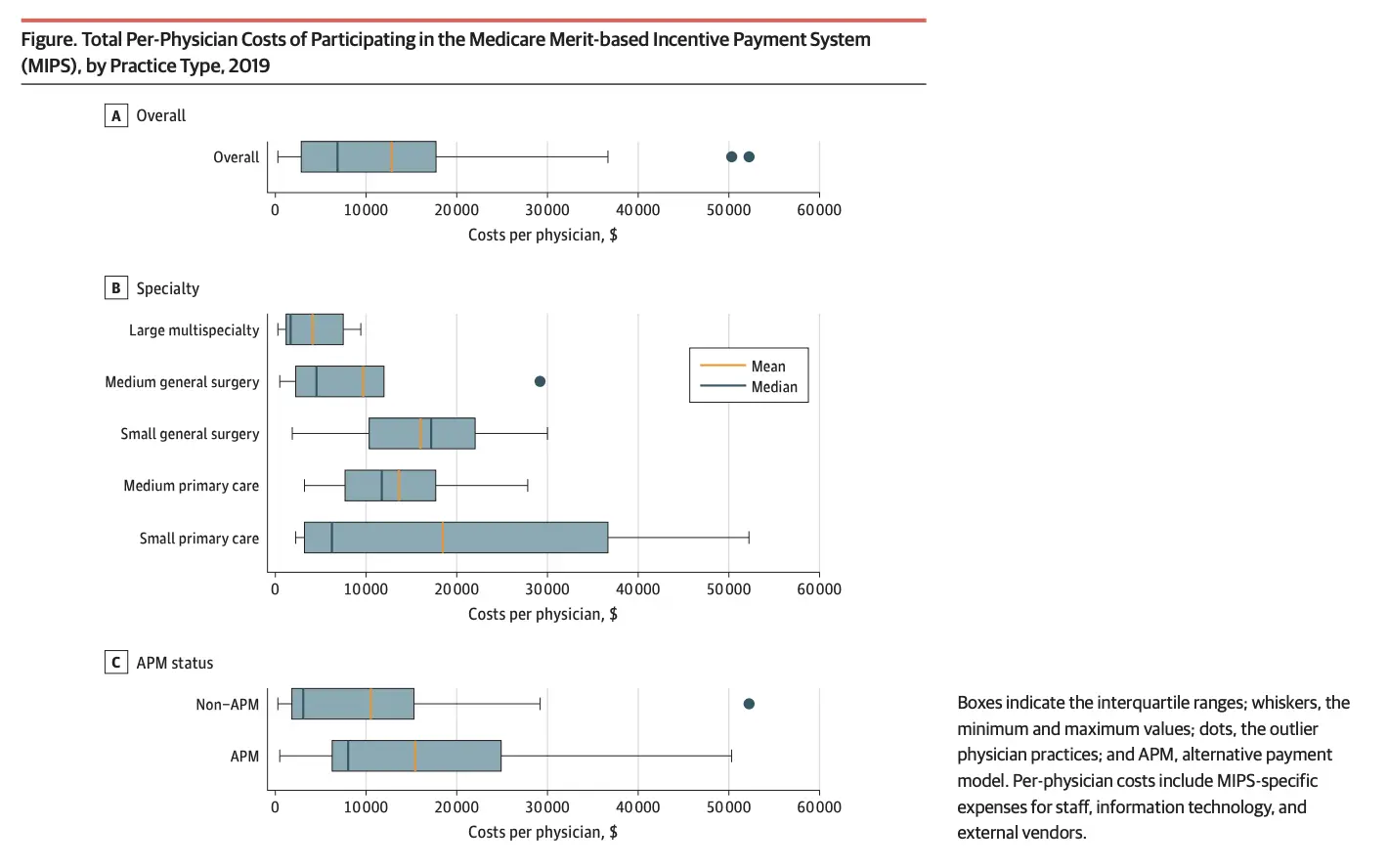
- My personal opinion from when I was running Flatiron’s program: I was surprised at the resources providers invested towards the program, despite the limited near-term upside potential. In 2017, the year I ran it, the upside was ~$4k per provider maximum. A provider's performance and upside payment depended on how the provider performed compared to every other provider, so even $4k was not a guarantee. I wish I better understood how providers justified spending on personnel and consultants to manage MIPS programs given what the payoff looks like. As the program has evolved, the downside risk has also increased (it’s a 9% penalty now), but for the first year or two, a neutral payment ($0 reimbursement + $0 penalty) could be achieved through a very basic submission. I was always curious why more people didn't take the “net neutral” in year 1 and spend this budget on other projects. A recent study actually validated this, showing that the administrative/cost burden is quite substantial.
{{interlude 3}}
4) Well...we can talk about scaling a CS org! How did you think about OKRs/KPIs, delegating responsibilities, etc.? Did that change over time at Oscar?
One of Oscar's initial differentiators was the fact that you could call into Customer Service and get in touch with a human almost every single time, and this remained an important characteristic to maintain. As the org continued to grow, this meant that our staffing models became more and more complex - how many people we needed on the phones each day, when team members could work on special projects outside of answering the phones.
We also wanted to optimize for "first call resolution" - or the likelihood that a person's issue could be addressed and resolved the first time they called, with no escalation. With scale, this meant that our training became more sophisticated and we needed to continue building out resources to support the front line team. Over time, we started to think about the role that our highly engaged, high touch service model could play in a member's care more proactively. This was the start of the concierge team model, which still exists today.
We built out "pods" consisting of clinical and non-clinical team members, who were assigned to panels of patients. These pods could conduct proactive outreach to members based on activity that we saw in our system. After I left, a focus of the ops teams became thinking about how to increase the volume of members per panel, demonstrating that the panels were handling member queries and issues even more effectively. I imagine this, in addition to the team's relocation to Tempe from New York, were some of the biggest shifts that the team experienced.
Customer Support teams are great for extending the brand or 'human ' side of an organization, but I learned a lot about people management in this role, too, especially because the Service team was by far the biggest in the organization. I remember when we hit a certain size, we started giving team members ChromeBooks instead of MacBooks, when everyone else in the company had Macs. This may seem like a reasonable cost saving move, but unspoken changes like this can have a real impact on how a team views itself within an organization. This was a huge takeaway for me and something I'm constantly thinking about within my own teams / organizations.
As for why the human element was important for Oscar (e.g. why we elected not to use chatbots or something analogous), you have to remember that Oscar was the first of its kind insurance company, trying to redefine an industry riddled with opacity. We prioritized having friendly, engaged, and fast answers to our customers because it was the only way we were going to begin the trust-building process. What’s exciting is to see the influence that this had across the industry. Even today’s chatbots are infused with a human touch, to make us feel more connected to the company we’re speaking with.
5) Switching gears a bit to Cedar. I'm a novice at billing and payments, but what makes healthcare billing/payments so much different than other industries? Are there surprising ops challenges you've come across?
In general, there are many ways in which we as consumers pay for things: ecommerce, point of sale, calling in and providing your credit card information. Oftentimes, business models will align with one - maybe two - of these. For example, if you're a brick and mortar store, you need to support point of sale, but not ecommerce. If you're an online retailer, the opposite is true.
In healthcare, and particularly at Cedar, we're working through all of these payment flows, which each come with their own suite of technical requirements and specifications. Folding all three of these payment flows into one offering (and this is before getting into things like payment via credit card versus ACH versus ApplyPay....) is extremely complex.
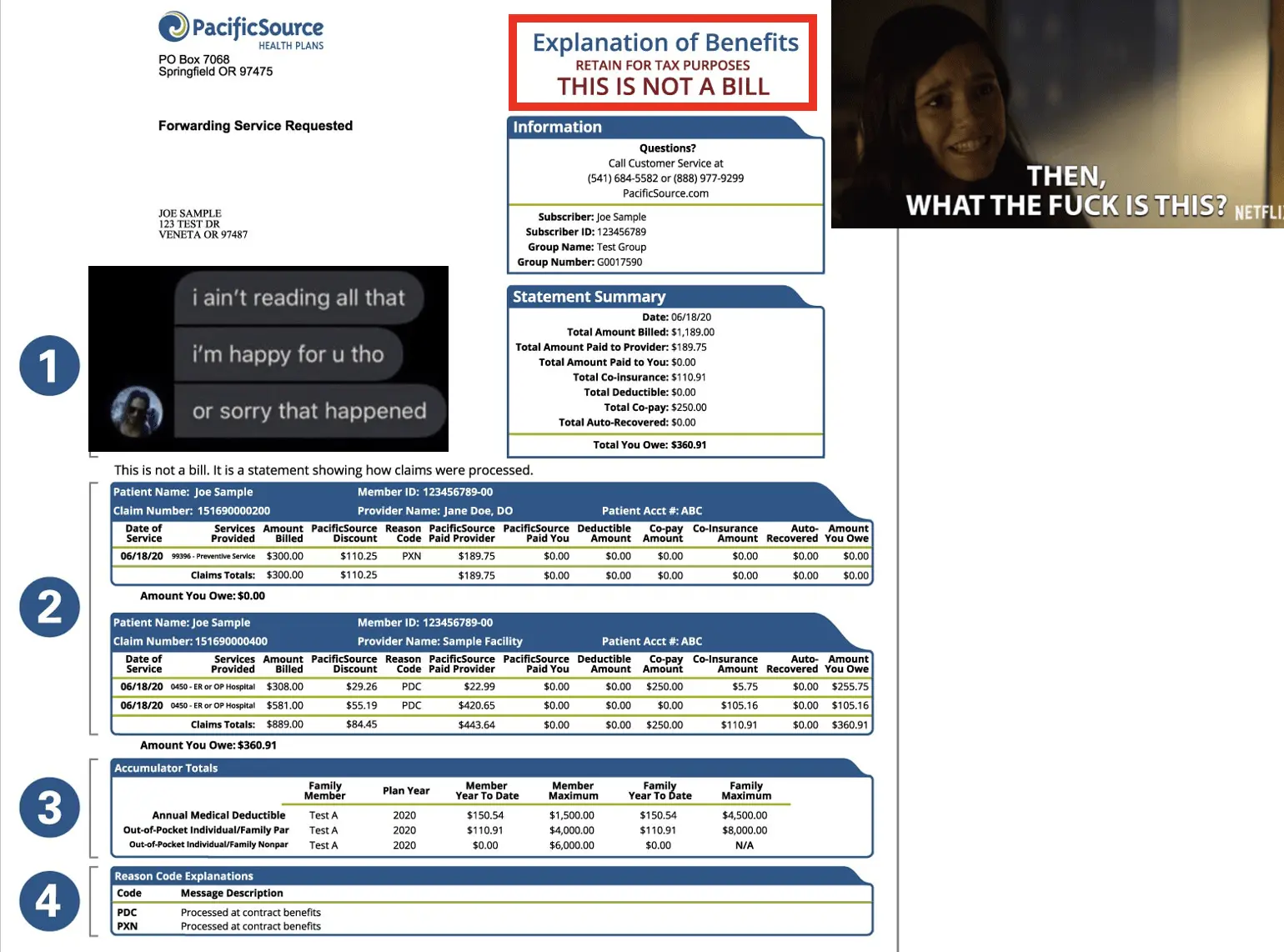
The integrations are also incredibly complex. At the risk of turning this into a fintech interview (which I suppose could also aptly be titled Out of Pocket), think for a moment about all of the different entities involved in communicating to you how much you owe or can expect to owe on your medical bill. Your health insurance company is sending an Explanation of Benefits. Your health system (via Cedar!) is sending you a bill. Maybe you have an HSA. Maybe you’ve had five different visits in the past month or you just had a really complex hospital stay that involved a number of different providers, not to mention the fact that the physicians in a hospital will bill separately from the hospital facility itself.
Now think about making a payment related to any of this care. Maybe you paid at the front desk when you checked in. Maybe you paid after you received your second text-notification from Cedar. Maybe you called your doctor’s office to request a refund because they overcharged you, and maybe they’ll refund you via check even though you paid via your HSA card.
Point is, there are a lot of transactions that need to be reconciled across different intervals of time and different technical systems that record and communicate these transactions uniquely. Historically, our healthcare system has put the onus on the individual to own this process. That’s ridiculous because if they have a high volume of bills to manage, it’s likely that they’re navigating an even more complex healthcare situation. This patient shouldn’t need to spend time combing through piles of paperwork; they should have a simple way to pay their bill that handles all related complexities on their behalf.
6) Why does it take so long for me to find out what my share of the bill is after I see a doctor?
As I thought about my response to this question, a Rube Goldberg machine came to mind. There are a ton of different steps in the process after you seek medical care. Here's a simplified way of thinking about it:
- a billing team codes the visit in a claim
- the claim is submitted to the insurance company via a clearinghouse
- the insurance company processes the claim
- the payment information (including what an insurance company pays the provider & what you as the patient owes) is sent back to the provider
- and then a bill is generated.
Each of these steps might take days or weeks, and it's dependent on how the claim is coded, if there are any denials or issues, etc.
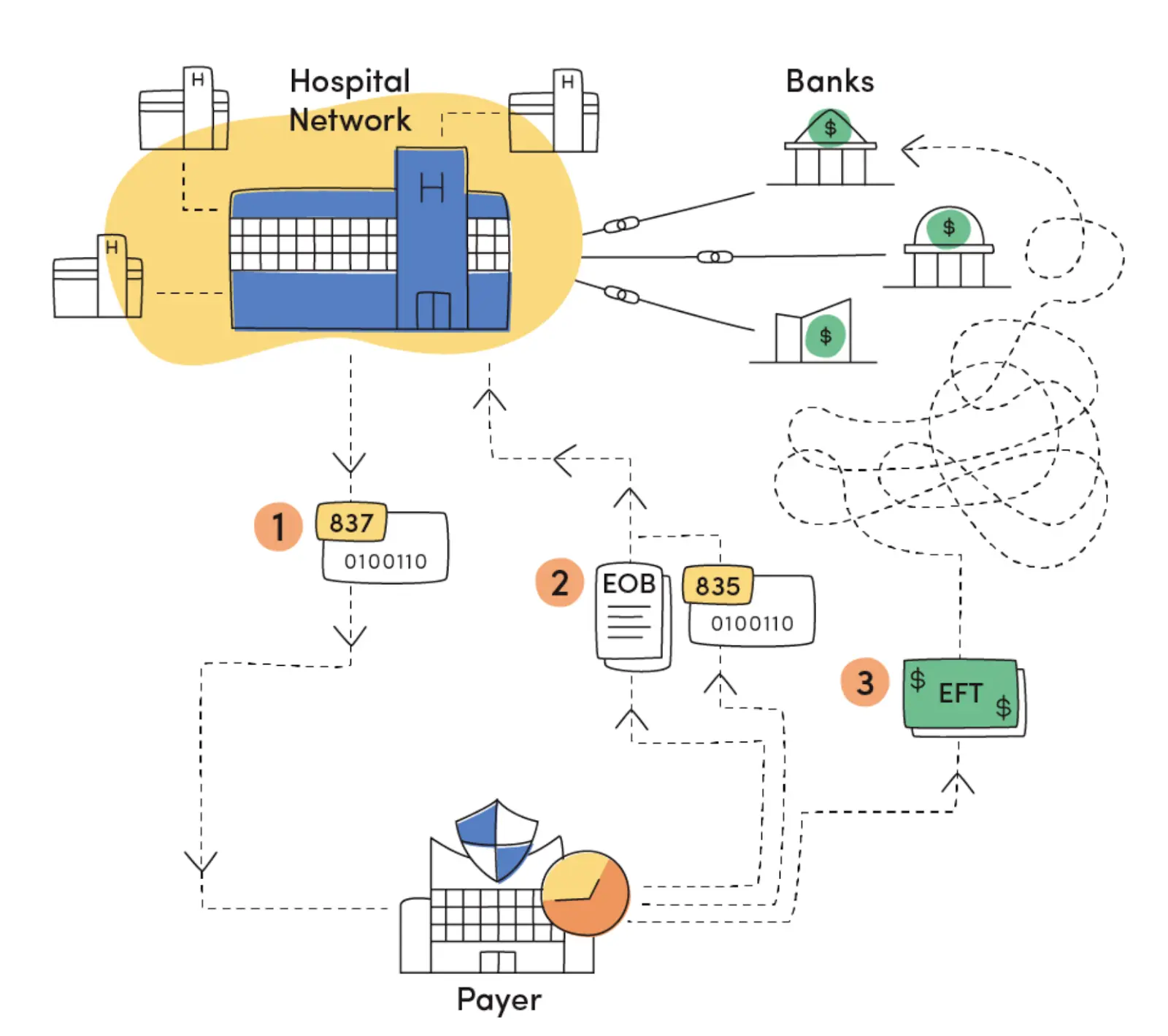
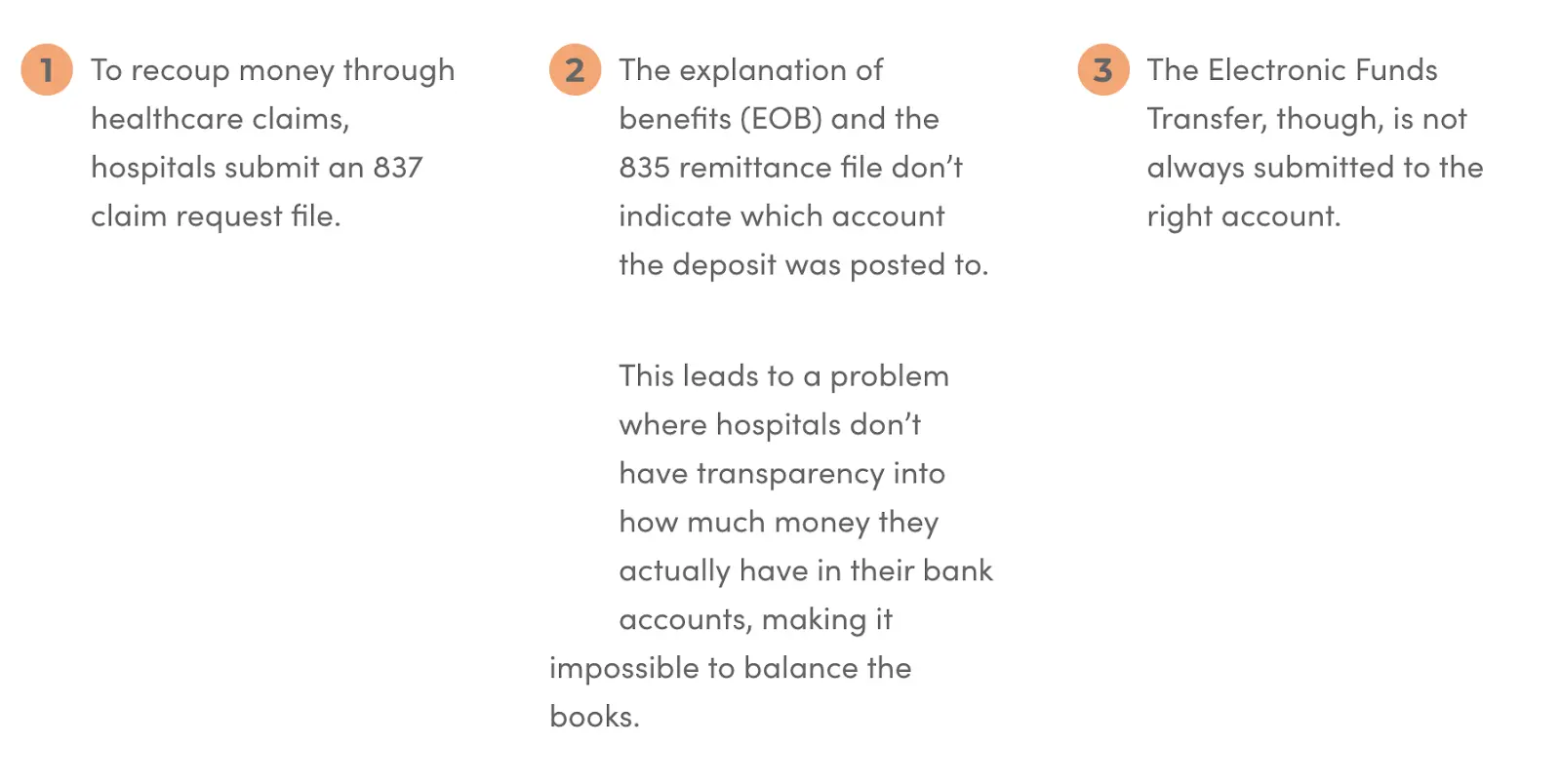
Avelead does a nice job explaining this web from the perspective of the provider ← → payer relationship, which of course has an impact on the final amount that a patient is billed and/or owes. To summarize this process:
- A provider submits an 837 file to a payer
- The payer eventually pays funds via electronic funds transfer (EFT).
- The information included on this final payment (an 835 ERA) may not match the information on the original 837.
- When payments are posted, they may be posted in one amount that reflects many, many smaller transactions (without posting the breakdown) or money may be posted to one of a number of a health system’s bank accounts, making it hard to trace and/or reconcile.
One of the things that makes me most excited about Cedar & OODA recently joining forces is the opportunity to tighten the relationship between health systems & insurance companies. For consumers, the combined entity will be able to accelerate the speed and accuracy with which a person can see what they owe without them needing to act as the intermediary between their health insurance company and doctor. This benefit brings me right back to my Oscar days, when we would have members call us asking about an issue with the bill they received. Nine times out of ten the response was “You’re going to have to ask your doctor to look into this to re-submit the claim with new billing.” Usually, the member was calling us because their doctor told them to call their insurance company. This lack of connectedness is an awful experience for the person taking time out of their day to get an answer to what they thought was a simple question. Needless to say, I’m ecstatic about the impact Cedar will have on this space.
7) So I've read lots of stories about hospitals and collections agencies - when does a hospital actually send a bill to collections? And is that money they expect to actually get back or are they selling the debt?
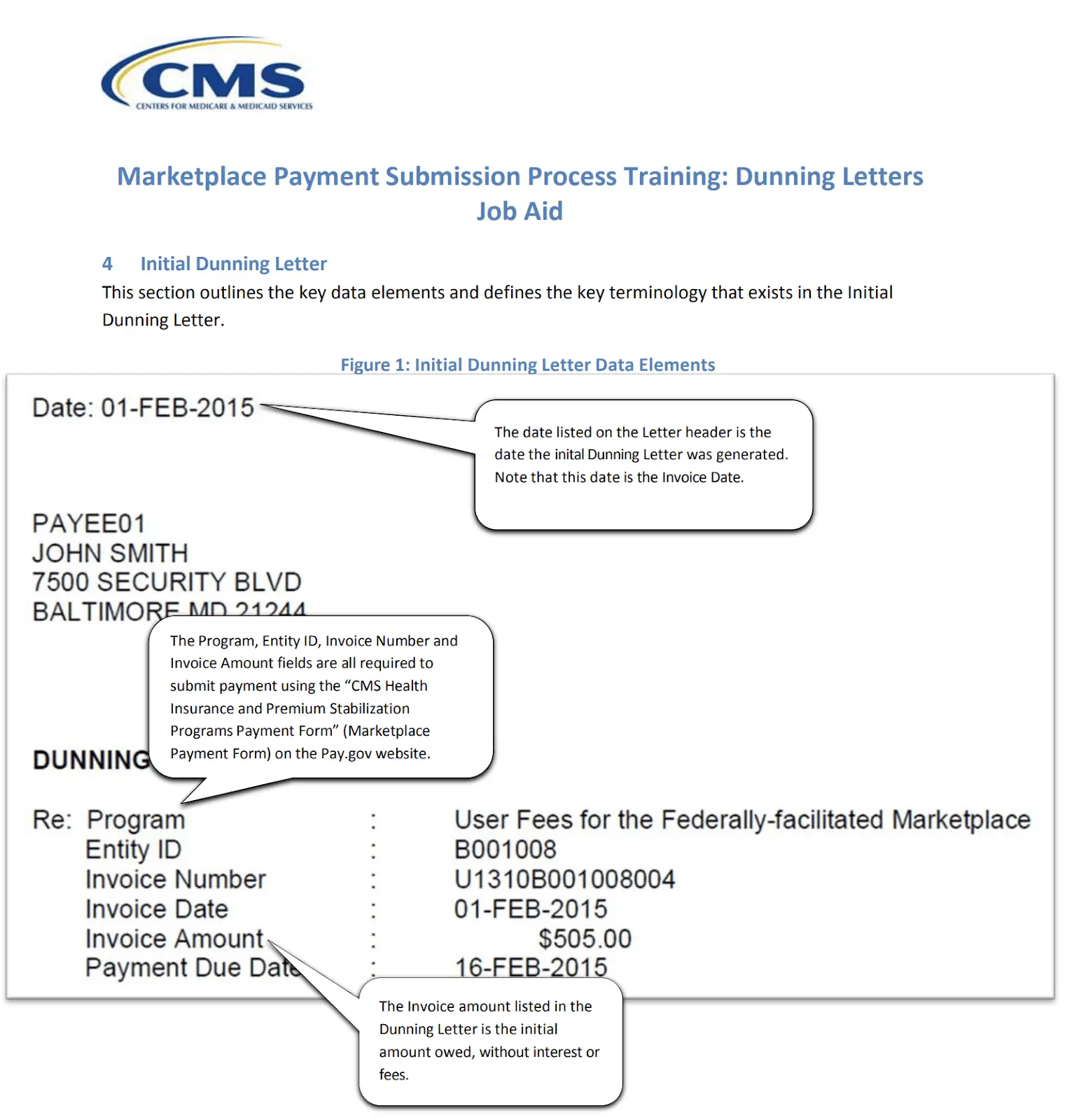
Great question. It really depends on the hospital. Hospitals send bills to patients on set intervals known as the Dunning cycle, typically in 30, 60, 90 day cycles, though the actual timing of these intervals are specific to a hospital or system. After the receivables have “aged” beyond where the hospital is collecting payment from patients - for example, when a bill reaches 120 days in the cycle - the hospital may decide to transition the bill to someone else who will be on the hook for collecting the money.
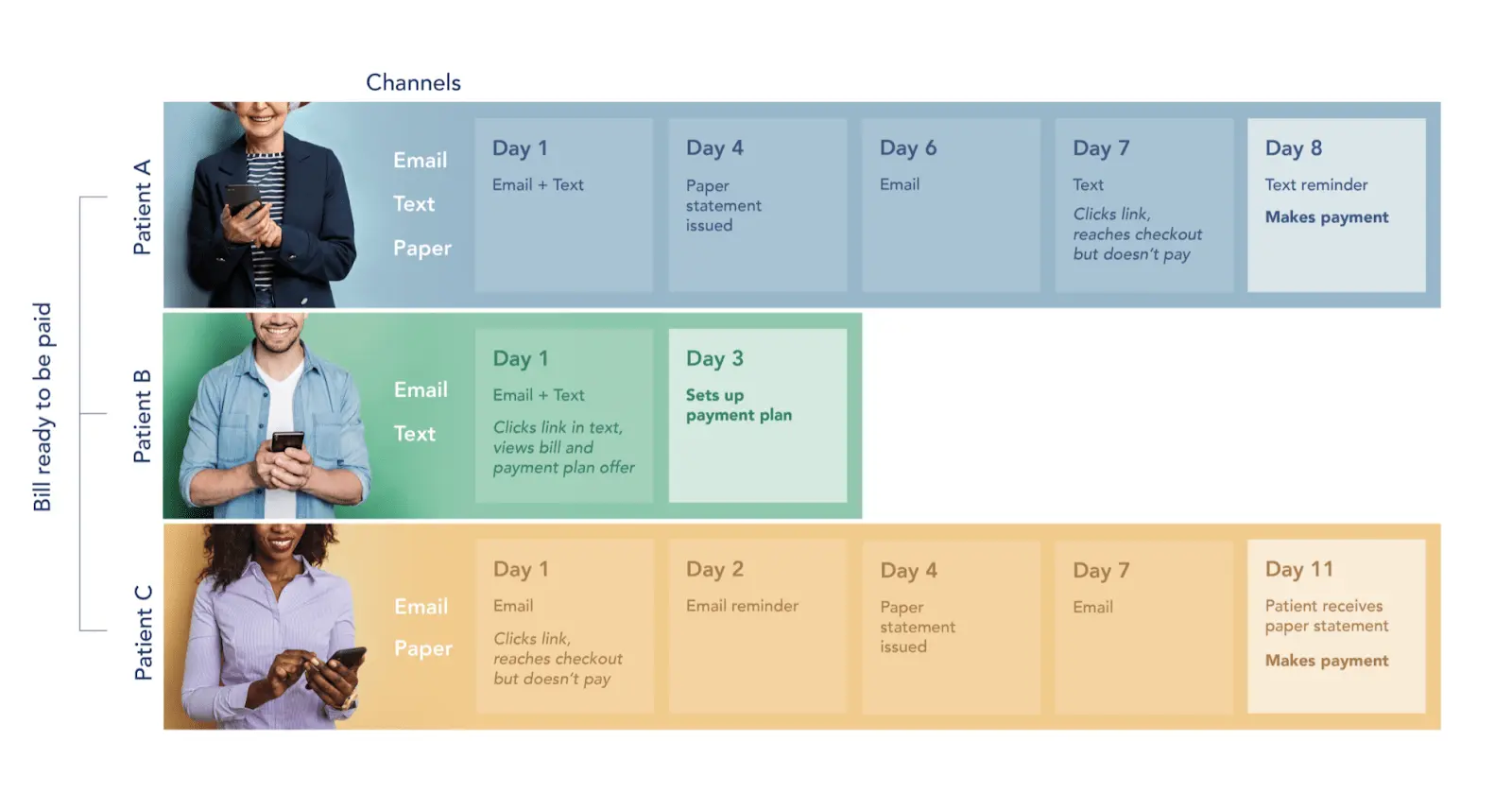
Cedar partners with health systems, and our patient billing platform actually has the goal of making it easier for people to pay their bills to reduce the likelihood that they are sent to collections at all. One way that we do this is by shattering the existing 30/60/90 day billing cycle and engaging people on different intervals:
But what happens to the money when people still don’t pay their bills? There are a few different ways that a health system might manage this, and again, it varies depending on the organization. Some entities might partner with an organization who will take money off of the health system’s balance sheet and help them collect by underwriting the risk against the health system itself. If the partner organization is unable to collect after a predetermined period of time, the outstanding money will be returned to the health system’s balance sheet (at which point they could transfer the money to a debt collector). This is known as recourse lending.
Other entities might partner with a solution who is actually underwriting the specific patients, which could result in higher interest rates for the individual (health systems have strong credit ratings). These organizations will own the risk long-term, meaning they’re not returning the receivables back to the balance sheet. Spoiler alert: this is called non-recourse lending.
8) If you weren’t at Cedar, what company would you be starting? What’s an opportunity in health insurance/payments/etc.? You can give me your second best idea if you wanna keep the best one for yourself :)
I’ll give you my best! When I was in business school, I spent a ton of time researching an idea about expanding access to doulas. A few years ago, the New York Times kept publishing articles about the benefits of new mothers working with doulas to address postpartum care. This intrigued me, and I started to dig into why there was this incredible resource for both new parents as well as expecting parents (doulas can be used throughout prenatal, birth, and postpartum) that was being positioned as some breaking discovery.
I became really curious about the birth journey and birth experience and found that there is a whole body of research demonstrating the tangible impact that doulas can have on the birth experience: this paper specifically talks about reductions in preterm births and C-sections. I started to learn more about the challenges that doulas face as I looked into why they are also such an underutilized resource. Eventually, I developed an idea (with many classmates along for the ride!) for a tech platform that would enable doulas to manage their businesses (marketing, payments, taxes - basically all of the elements they’d rather toss to the side) that would also serve as a marketplace for new parents to search for and connect with doulas. I’m less keen on the marketplace element, but I do think there’s something worth unpacking on the tech platform side. And there are so many companies popping up in the space! I love the teams at Mahmee and Oula.
Bonus: You recently launched an initiative called 81grants to help women of color with salary negotiations. Can you give me the mini spiel on what it is and how it's going?
Yes! 81cents is my best friend Jordan's company, which she started over 3 years ago while in business school to solve the gender pay gap (the company’s name is a nod to the ratio of dollars that women earn on average compared to men, and it’s important to acknowledge that this number looks even worse for women of color).
It works like this: 81cents clients purchase a market value report, and a client inputs their current comp package or potentially a future job offer. Once submitted, 81cents arranges for a team of advisors to weigh in on the offer based on their own knowledge of the role and market. This arms clients with better data to successfully negotiate compensation. On average, 81cents clients see a 17% increase in total compensation. The 600+ clients who have worked with 81cents have earned over $3 million in additional compensation.
Last summer, Jordan and I were discussing that the pay gap is even worse for women and people of color, and we wanted to do something about it. Jordan and I spent the fall of 2020 launching "81grants", a division of 81cents that provides complementary market value reports to women of color who might find the reports to be cost prohibitive. By removing the cost barrier & arming these women with the same tools, we hope to make a small dent in closing the disproportional pay gap that women of color experience. We’ve given out 65 in 2021. Our target for the year was eighty-one. Huge win for our incredible applicants.
Thinkboi out,
Nikhil aka. "Friends With Explanation Of Benefits"
Twitter: @nikillinit
If you’re enjoying the newsletter, do me a solid and shoot this over to a friend or healthcare slack channel and tell them to sign up. The line between unemployment and founder of a startup is traction and whether your parents believe you have a job.
{{sub-form}}
Interlude - Apply to Knowledgefest! And healthcare 101 starts next week!
See All Courses →Don’t forget the application for our Knowledgefest, our healthcare software engineering conference IS LIVE.
If you work in healthcare ops, you want to be here. This is where you learn playbooks, see what other ops people are doing, and build your network. It’s year 5 and we sell out every year - applications are due end of month.
And if you feel like you really need to get up to speed on how healthcare works, then you should let me teach you at Healthcare 101starting next week!This is for anyone hiring teams of non-healthcare people that need to get up to speed quickly (in 2 weeks) - we do group discounts too hit up ya boy. You’ll even learn how to make memes.
.png)
Get Out-Of-Pocket in your email


