




Rethinking organization structures
Get Out-Of-Pocket in your email
Looking to hire the best talent in healthcare? Check out the OOP Talent Collective - where vetted candidates are looking for their next gig. Learn more here or check it out yourself.
 Hire from the Out-Of-Pocket talent collective
Hire from the Out-Of-Pocket talent collectiveFHIR 101

Featured Jobs
Finance Associate - Spark Advisors
- Spark Advisors helps seniors enroll in Medicare and understand their benefits by monitoring coverage, figuring out the right benefits, and deal with insurance issues. They're hiring a finance associate.
- firsthand is building technology and services to dramatically change the lives of those with serious mental illness who have fallen through the gaps in the safety net. They are hiring a data engineer to build first of its kind infrastructure to empower their peer-led care team.
- J2 Health brings together best in class data and purpose built software to enable healthcare organizations to optimize provider network performance. They're hiring a data scientist.
Looking for a job in health tech? Check out the other awesome healthcare jobs on the job board + give your preferences to get alerted to new postings.
New org structure, who dis?
In part 1 of this series, we talked about alternative financing mechanisms for digital health companies. Today in part 2, we’ll talk about whether different organization structures might be worth exploring for healthcare companies.
*Reads Coase’s Theory Of The Firm once*
Okay so here’s the problem with “companies” bro...
Corporate structure
I think a lot of people in healthcare across the board are getting kinda sick of top-down decision making.
On the large company side, there’s a division between what management thinks is the right thing and what frontline workers think is the right thing. The tension between frontline staff and hospital admin is so thick it’s basically sexual.
Startups, on the other hand, are all about speed. How fast can we grow, hit the next milestones, fundraise, etc. In order to do that, top-down decision making has been the optimal governance structure - the C-suite makes decisions and then that permeates down to the rest of the org. Everyone else gets to do the fun KPI planning that fits into those decisions and will definitely still be relevant in 3 months. Definitely.
However, there are downsides to this model that are now becoming clear. The reality is that the incentives aren’t aligned between employees, founders, and investors. The very tiny bit of equity you get as an employee is a pretty shit deal. And exiting to make your small amount of equity worth something is tough when the company has already raised a ton of money. Plus, maintaining product quality and operations while blitzscaling is extremely hard.

In both small and large companies, the top brass and investors make decisions about how the company finances itself, when it chooses to exit, and where it chooses to spend money. Everything else comes downstream - how you think about product roadmap, metrics to optimize for, headcount expansion or reduction, sales cadence, etc. But employees have no real say in these decisions. Wouldn’t you feel pretty bad as an employee if you got laid off after your founder sold ~$100M of their stake a few months earlier? Or if you were told to do some gray area ethical thing you didn’t feel comfortable doing for the sake of growth to hit the metric for the next round? Or if you didn’t get hazard pay during COVID but the hospital is planning an expansion?
Now that the economy is getting more precarious, people are aware of the tenuous state of their employment and the decisions that led there. And everyone is a bit more adamant about getting the financial value they think they deserve today, because I’m this close to needing to buy eggs in four easy payment installments.
Are there different ways companies can structure themselves to include more workers in decision-making and closer to the money?
Some Alternate Org Structures
It’s 2023, I think companies should feel comfortable exploring their structurality 🙃. Potentially in ways that give more governance and financial upside to the people involved in building the company. A few options:
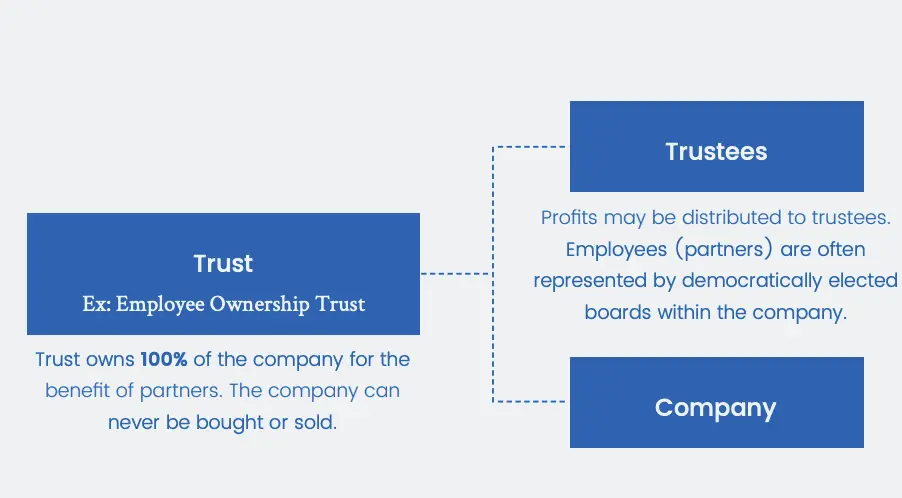
Employee Ownership Trust / Succession - There are a lot of companies with interesting structures that utilize trusts to prevent outside shareholders from only optimizing for profit extraction. One interesting version to me is the Employee Ownership Trust model, which UK retailer John Lewis implemented. In this model, distribution of profits go to employees, which seems to be ~15% of annual salary. More importantly, they have the ability to vote or fire people elected to the board and establish a Partnership Council with elected representatives that are the voice of the employees. All major company decisions need to get approval from them.
Ironically, the last time the UK tried to give us a system of governance we…had a revolution and created a system that had more representation. It’s in the Prince Harry tell all.
Maybe front-line staff would feel like they had more of a voice if a hospital was structured like this. For example, one of the big wins highlighted by the nurses union in Minnesota is they’d have a say in what staffing levels looked like. If the employee pool were the ones that elected the board, there might be fewer fights between the unions and hospital administrators.
Cooperatives - Cooperatives (aka. Co-ops) are organizations that are owned by their members. There are lots of ways to structure them, but here are some common examples.
- Consumer Co-Ops - This is typically a business “owned” by the people that actually use the goods and services. The Park Slope Food Co-op is a grocery store you can’t go to unless you take a shift working for the store, and it has a town hall where people vote on what to stock, % markup of food, etc. REI is a co-op where a portion of dividends are paid back to their members. This ends up reducing their marketing spend, because people who shop at REI won’t shut the fuck up about it.
- Worker Co-ops - This is when employees collectively own a company and make decisions as a group. Usually, this process requires employees to work a certain number of hours, get voted in, and buy shares in the business. This structure is more popular with breweries, coffee shops, bakeries, etc. You can find a full list of them here.
- Producer Co-ops - This is more common among farmers or people who all produce a similar product. Frequently, they’ll use their group’s leverage to negotiate down prices of inputs + expand markets they sell into, but also, they’ll share facilities for processing and distribution. For example, Land O’Lakes is a co-op of dairy farmers and does everything from distributing into retail stores, purchasing trucks, access financing, and even health benefits for its members. I’m sure they have excellent heart disease programs, because irony knows no limit in US healthcare.
There are already some inklings of this in healthcare. There used to be several health insurance co-ops that got rekt because the government didn’t pay their promised risk corridor payments. For companies that need to get patient insights, there are some patient-owned co-ops like Savvy . Independent Physician Associations (IPAs) look like producer co-ops for independent physicians because of how they negotiate with insurance and other vendors. There are several member-owned group purchasing organizations like HPS that negotiate rates for supplies and create standardized RFPs for members. How come there isn’t a member-owned PBM co-op that passes the rebates directly to patient members?

Co-ops are still pretty sparse. Maybe a template or easy way to set up a co-op would lead to more practice co-ops, insurance co-ops, etc.
Decentralized Autonomous Organizations (DAOs) - Could a hivemind of people in a group chat build something if there were no singular CEO? DAOs are essentially groups of people on the internet that can pool money together, propose where the money should go, and then contribute to the project that is awarded the money. The DAO basically functions as a company, but there’s no singular CEO, anyone can pitch ideas, and the rest of the DAO can vote and contribute to it. There’s some crypto stuff that ensures funds actually go to the right places and tracks voting to wallet addresses. I know half of you reading this are wondering if I’m having a stroke.
In DAOs you can see someone’s entire voting history, you can limit votes to members that have certain characteristics (e.g. only people that showed up to the last few votes, own a specific NFT, or only people that have a certain amount of tenure), and you can delegate your votes to other members that you trust if you’re not going to be there.
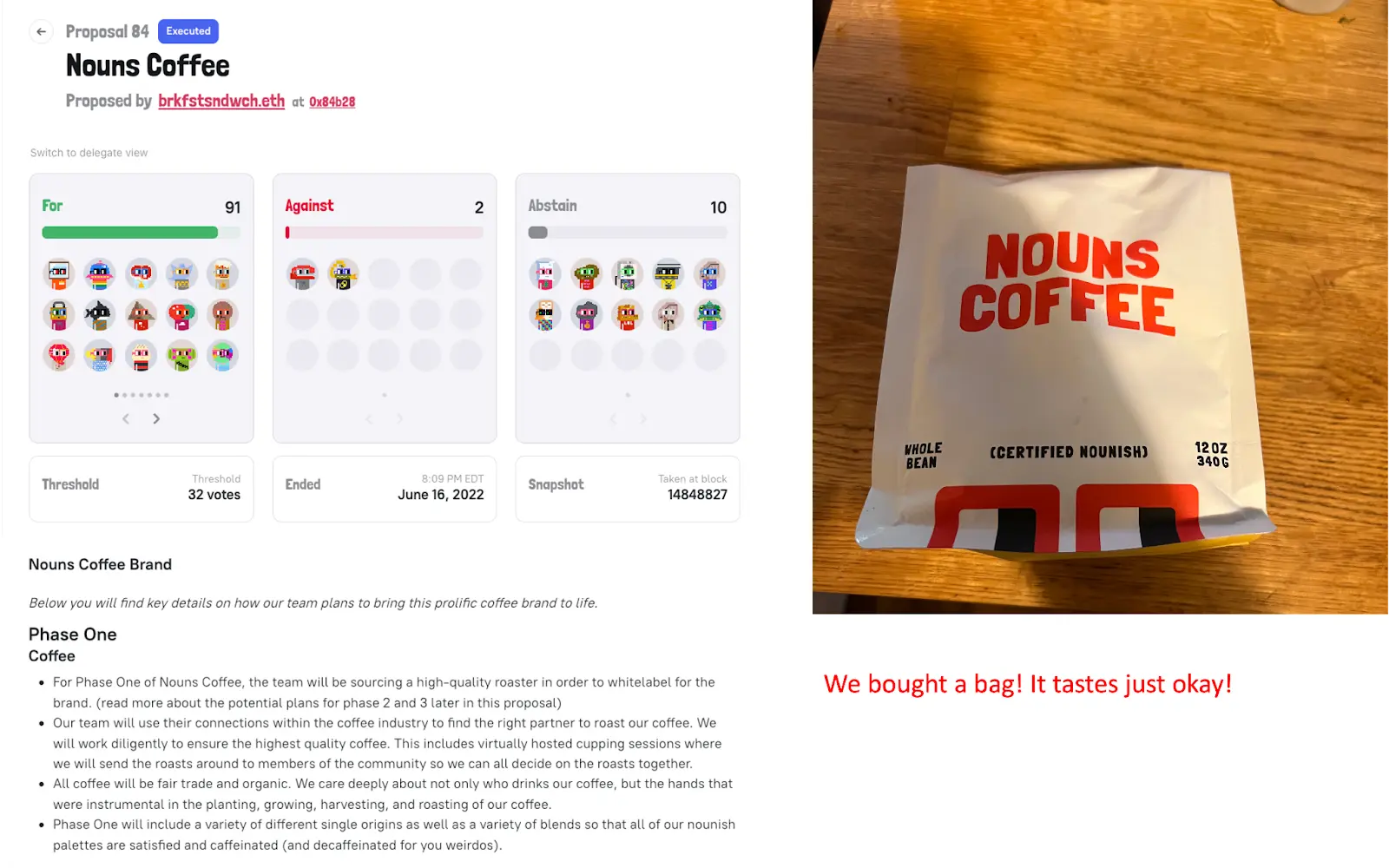
Here’s an example in “nouns DAO” where someone proposed making a coffee brand with the DAOs image on it and explained how the funds would be used. There was some discussion, people voted on it, and it got created. I actually had a bag of it, and even though it kinda tasted like ass– it did in fact exist! A group of randos on the internet had a mechanism of coordination to create it without a C-suite making the decisions, which is pretty cool.
In the past I’ve highlighted how this model could be useful for peer review, picking drug assets in a pipeline, and peer-to-peer insurance. But honestly the more I think about how many things in healthcare require voting from a representative population that doesn’t ACTUALLY feel represented, the more I wonder if DAOs have even more use than we think. For example, a small committee of 32 physicians is supposed to represent all physicians and decides how physicians should get paid for their services. This might actually work better as a DAO with delegated voting.
Franchises - If you don’t want to take the full risk of starting your own business from scratch, you can get a “business-in-a-box” from a franchise. A company will let you borrow their brand, train you on how to run your local version of the business, get you the supplies needed, group negotiate across the franchises, lend you money for things like equipment, and more. Companies like Mcdonald’s truly have the business and operations down to a science. They set it up for you; you just have to run it.
In return, you’re usually paying the parent company an upfront fee, a portion of royalties from the store itself, and then a bunch of other services you can choose to pay for. Both parties usually agree on certain “quality control” things to make sure you’re not tainting the brand, and contracts between you and the parent company can be long (like 10+ years long).
Fortunes can be made doing this correctly if you’re good but it’s pretty cutthroat. There are Subway sandwich dynasties in Jersey that’ll put a footlong hole in your kneecap if you cross them.
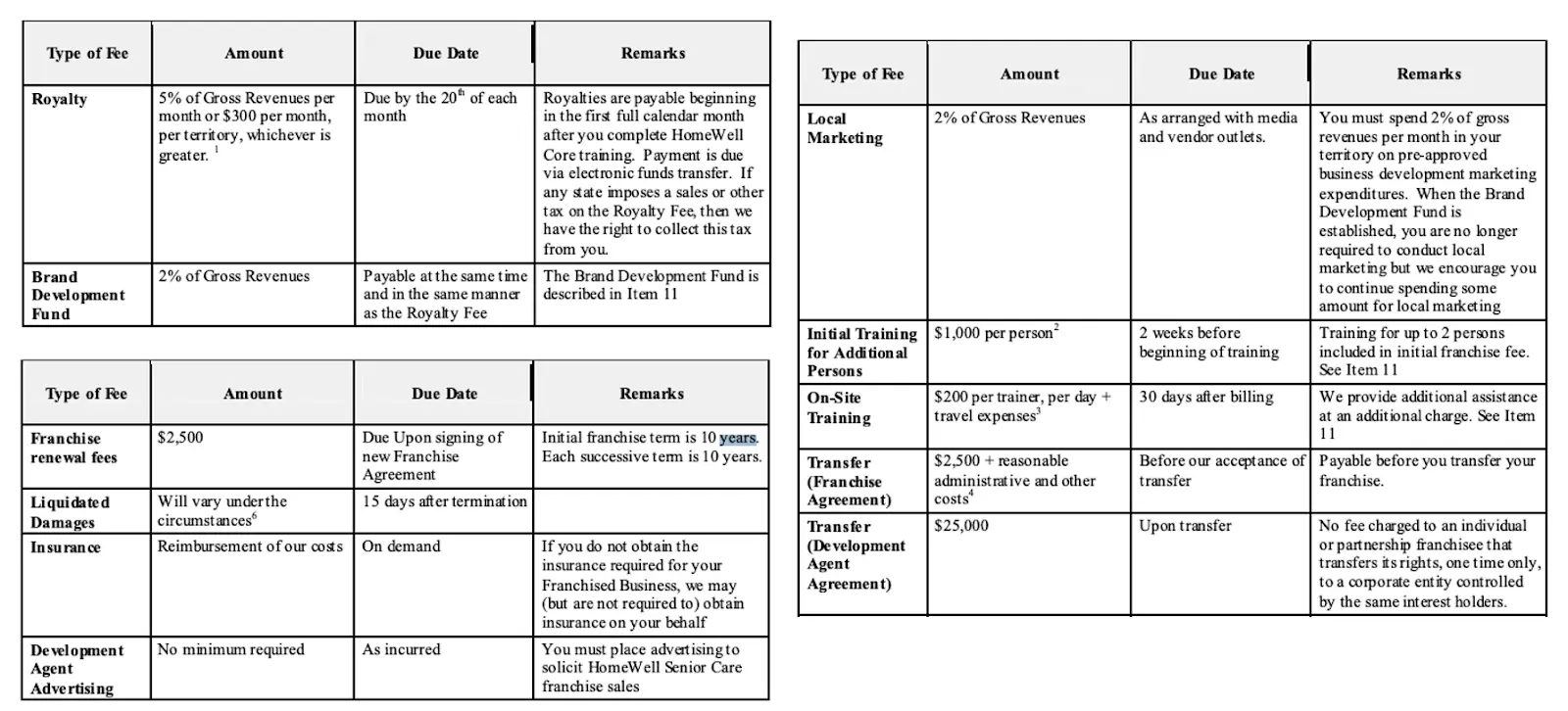
Franchising isn’t really a new idea in healthcare. There are tons of franchise opportunities from home care agencies, to nurse staffing, to physical therapy clinics, etc. Here’s an example of some of the fees you would pay to a senior care franchise: $39,500 upfront, 5% of gross revenues, another 2% of gross revenues for brand development, add-on fees for training, and a 10-year contract that can be renewed.
I’m gonna keep it real with you all. I went through the process to “apply” to some of these to see what the materials look like. A lot of these franchises are shady as hell and are most likely making money off the upfront fees vs. actually setting people up for long-term success. I’m more confident I’ll get my investment back from robocall spam than a few of these home care franchises.
Even though franchises aren’t new, I wonder if there’s room for more franchising models. Maybe ones where the process to qualify doesn’t feel like a timeshare sale. For example, Oak Street franchising out to docs that want to go independent but don’t want to start from scratch. Honor seems to have bought a company that does home care franchising and combines it with their back-office tech. Yoni Rechtman wrote a good post about franchises and how they might work in healthcare here.
In fact, why don’t payers offer docs who want to go independent something like this? Give them reimbursement contracts in hand + services to help them find their first spaces. Maybe this is something Optum does in the future, or maybe I can convince the Taro* team to make Direct Primary Care franchises for interested docs.
*Disclosure: I’m a value-subtract investor.
Partner networks - Out-Of-Pocket itself is an experiment. I am a one-person company (read: lonely) but I’m bringing partners in to run different business lines underneath the larger brand umbrella (courses, conferences, etc.). They decide the cadence, pricing, content, etc. and we do a profit share. Sure this business probably won’t become a billion dollar company, but the pace of growth is sustainable and everyone involved feels more ownership over their slice. The Krishnan-Chan-Zuckerberg hospital won’t be from that Out-Of-Pocket money.
My company structure looks a little like franchising. But instead of taking the same business and using that playbook to replicate in new areas, it’s meant to support people that want to start new business lines under the brand. Businesses now can produce a lot with very few people thanks to tech - which I think might make this small-teams-per-product-profit-share possible. Extremely online people have been referring to this as a “personal holding company” where a lot of different cash flow generating businesses live under the umbrella of one person’s brand. But that term sounds lame and is mostly used by people that type.
On the internet.
Like this.
So I’m not using it.
Maybe some of the healthcare and physician creators on TikTok, Instagram, etc. (which I’ve talked about before) could set up similar structures to run other parts of their business.
{{interlude 3}}
Are these better structures? For healthcare?
It’s worth calling out the specific tradeoff you’re making in these kinds of employee-friendly structures.
- There can be a diffusion of responsibility which leads to slower decision-making, more meetings needed to reach a consensus, less high-risk high-reward choices, and more groupthink. This article talks about how employee-owned co-ops keep arguing about ketchup dispensers and took multiple years to approve a patio. How would they respond to something like COVID without top-down governance that requires a lot of moving parts working together under a singular plan?
- Getting external financing and working with other enterprises at all is difficult, which makes businesses with large upfront expenditures difficult to get started. People who are investing or running a pilot with you typically want a single person responsible for making the business successful.
- Actually tracking who does the work is hard, and preventing free riders might be an issue. I think this is solved by keeping the company smaller and more reliant on social pressure to get stuff done.
- The above also complicates how compensation works. Some places give raises based on tenure vs. output, which has its own set of problems. REI’s CEO got roasted in the Reddit AMA by the people that actually work at retail stores about compensation bands.
- Figuring out hiring + firing, how to bring on new members on, and their specific role in making decisions is much more difficult without a somewhat clear hierarchy.
- By working at one, you’ll get called a commie by people who have likely never left the US.
But I think what you might gain is longer tenure of members and more buy-in from people working at the organization. This would be especially important in industries where labor shortages are common, highly skilled labor is scarce, and people are motivated beyond just direct financial compensation. If only we knew an industry like that…
Rethinking corporate structure in healthcare could be uniquely important for a few reasons.
- I think decentralized decision-making is particularly important in healthcare because of the need to understand local nuances. Each state regulation is different, the local referral networks are different, the attitudes of patients in different areas/demographics are different, etc. Giving more ownership to people that understand these local nuances CAN lead to faster and more effective decision-making.
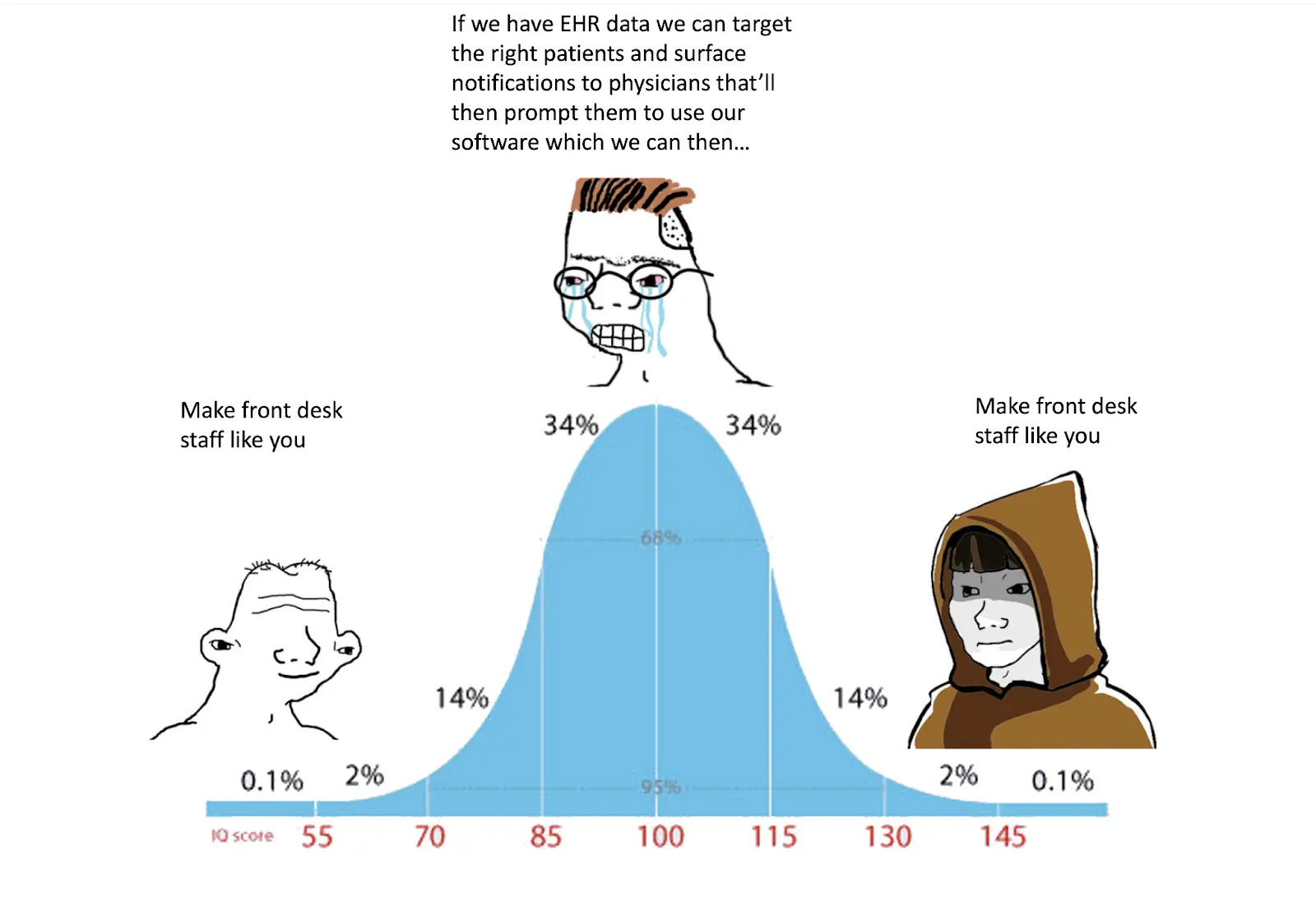
- The success of many models in healthcare is dependent on the people who are least likely to have meaningful ownership (patients, frontline staff, front desk, etc.). If a clinic needs to convert Medicare patients to Medicare Advantage, or requires consistent patient outreach to make sure care gaps are closed, etc., you need buy-in from the entire team. Companies will spend tens of thousands of dollars in marketing spend or software tweaks before realizing the key to getting physicians or patients on board is actually coffee/pastries for the front desk staff. Now imagine if that front desk staff also had equity and could vote on suggestions on how to improve processes.
- There are metrics in healthcare that we should care about societally that are at odds with our fiduciary duty. Member or employee-owners will theoretically care more about certain things that benefit the community, employees, patient livelihood, personal reputation, etc. that no “3 last names” consulting shop can optimize for (or just isn’t well measured). The current trend of clinician burnout is a direct response to trying to squeeze every ounce of productivity out of the workforce using metrics like RVUs. Is there an employee-ownership model that exists which can reduce this because the owners care less about pure returns?
Conclusion
I don’t think this is the only way companies should be structured. In fact I still think MOST companies will operate better as top-down centralized entities. But a little experimentation never hurt anyone, right?

I’m curious if anyone has thought about or experienced working for a company that has attempted a model with higher employee ownership/upside and what your experiences have been.
Thinkboi out,
Nikhil aka. “Top down, bottoms up, that the way I like to–”
Twitter: @nikillinit
Other posts: outofpocket.health/posts
Thanks to Elliot Cohen, Morgan Cheatham, Yoni Rechtman for taking a look at drafts.
{{sub-form}}
---
If you’re enjoying the newsletter, do me a solid and shoot this over to a friend or healthcare slack channel and tell them to sign up. The line between unemployment and founder of a startup is traction and whether your parents believe you have a job.
Quick Interlude - NEW COURSE ON FHIR! KNOWLEDGEFEST APPS DUE SOON!
See All Courses →So...what actually is FHIR? I get this question a lot, but there's never really enough time to explain it and also I would just mumble "technical standard" and walk away.
So we decided to do a standalone free FHIR 101 course in partnership with Redox! Over 3 days in August we'll go over the spec itself, how it differs from other healthcare information standards, and practical tips to build with it.
I wanted to call it FHIR fest but it got nixed. You can sign up for it here, it's FREE and it's 8/25-8/27.

And a reminder that Knowledgefest apps are due this week. If you want to be in a room with the best ops people in healthcare, you should apply like TODAY.
We sell this conference out every year - all workshops, learn how people are building and scaling in healthcare, application based so we only take the best. We have people from Commure, Clarity Pediatrics, Pomelo, and Waymark already coming, join the squad.

Get Out-Of-Pocket in your email


