




Healthcare in India
Get Out-Of-Pocket in your email
Looking to hire the best talent in healthcare? Check out the OOP Talent Collective - where vetted candidates are looking for their next gig. Learn more here or check it out yourself.
 Hire from the Out-Of-Pocket talent collective
Hire from the Out-Of-Pocket talent collectiveFHIR 101

Featured Jobs
Finance Associate - Spark Advisors
- Spark Advisors helps seniors enroll in Medicare and understand their benefits by monitoring coverage, figuring out the right benefits, and deal with insurance issues. They're hiring a finance associate.
- firsthand is building technology and services to dramatically change the lives of those with serious mental illness who have fallen through the gaps in the safety net. They are hiring a data engineer to build first of its kind infrastructure to empower their peer-led care team.
- J2 Health brings together best in class data and purpose built software to enable healthcare organizations to optimize provider network performance. They're hiring a data scientist.
Looking for a job in health tech? Check out the other awesome healthcare jobs on the job board + give your preferences to get alerted to new postings.
Eat, Pray, Healthcare
One of my favorite pastimes is complaining about the US healthcare system. But I need to expand my total addressable market, so I’m announcing that Out-Of-Pocket is now complaining about other countries as well going forward. The investors are thrilled.
More seriously, I think it’s always interesting to see how other countries' health systems are developing in parallel to ours. India has always been one I’ve wanted to dive deeper into because I am Indian and I should probably know more about this when people ask me lol.
But also because India is going through massive technological and demographic changes that is forcing the country to adapt its healthcare system. And it’s a great place to look at how a system adapts when it needs to be as efficient as possible to deal with the massive amount of healthcare demand for a giant population.
But it’s a little hard to learn about the Indian healthcare system as an armchair analyst sitting in the fast casual wasteland that is Williamsburg, New York. So I hit up my friend Amrit who is actually building a healthcare company in India.

We talk about:
- How the Indian healthcare system works generally
- The use of ayurvedic vs. allopathic medicine
- The role of technology in the Indian healthcare system
- Things that are working well for the Indian healthcare system and things that could be improved
- How badly he gets roasted for his American-accent twinged Hindi
- and more
Background, current role and latest cool project
Amrit: I’m a co-founder of Loop, a healthcare startup based in India. Our mission is to improve the lives of 10 million Indian families by 2030 through better healthcare.
To make this happen we are building our own healthcare system from scratch, starting with health insurance and primary care. Think Oscar Health meets One Medical.
And as CRO, I look after all things growth, including brand, marketing, and sales. So far we’ve enrolled 550k+ members on our healthcare plan.
I’m also a proud Illini. I grew up in Chicago and studied Finance at the University of Illinois-Urbana Champaign. Shortly after I graduated, my mom was diagnosed with a rare cognitive impairment. It was really tough, and just made it so much worse that we kept getting bounced around to different specialists and couldn’t figure out what was covered by insurance. So I started going down the healthcare rabbithole, and ended up joining Mayank and Ryan, now my co-founders at Loop.
Interesting Project: We are actively exploring how we can use ChatGPT to negotiate health insurance claims on behalf of our members in order to minimize their OOP expense. For better or for worse, legal frameworks like HIPAA do not exist in India, so we can move quickly and experiment with innovative new services like this.

How did you end up building in India?
Amrit: Our co-founder Mayank is from Pune- a “smaller city” of 6 million people just a few hours outside of Mumbai. In 2014 during our sophomore year in college, he was building an EMR for clinics in rural areas of India.
Technology has revolutionized every corner of the Indian economy- from education to entertainment to manufacturing. Everything is faster, better, cheaper because of software. Except healthcare.
Every 5 years for the last 2 decades, the cost of a hospital visit in India has doubled. The supply of good doctors is extremely low, and health outcomes are getting worse. Incidence of chronic conditions like diabetes and CVD is exploding.
Nonetheless, India is still about 30 years behind the US in terms of health insurance penetration and medical cost inflation which makes it an amazing moment to build. We have the opportunity to put the right infrastructure and incentives in place now to avoid all the massive problems we experience with US healthcare.
It was such an exciting challenge with so much whitespace that Ryan and I picked up our lives in the US and moved to Mumbai full time. A couple of “ABCDs” back in the motherland.
[NK note: For those who don’t know what an ABCD is…the struggle is real]
{{interlude 3}}
Can you give readers a basic overview of how the current Indian healthcare system works?
Amrit: It’s hard to talk about India as a single ‘healthcare system’. India is going through an incredible economic transition, but the divide between classes is still huge. The lowest earners mostly use public infrastructure, while the middle and upper class can afford private insurance and use private hospitals.
Let’s start with India’s bottom half. These people mostly reside in “smaller” tier 2 and tier 3 cities. (A small city in India is still usually millions of people). They face the age-old fight against communicable diseases like malaria, tuberculosis, dengue.

They mostly rely on public sector hospitals which provide nearly free healthcare services. There are more than 10,000 government-run facilities across India. But these facilities often face challenges with doctor shortages and bad infrastructure. The lines are super long, and to get an appointment you need to show up early (5 am) and wait in a queue.
It’s really difficult to deliver good care in every corner of the country. Sadly more than 200,000 Indians still die from tuberculosis every year, despite the fact we’ve had a cure for it since 1950.
For the middle and upper class (referring to the top 400m out of 1.4 billion) the story is entirely different. This group mostly deals with chronic conditions like diabetes and hypertension. Last year, India was recognized as the “Diabetes capital of the world” with 80 million diabetics, more than 2x the amount in the US.
India also has one of the highest burdens of cardiovascular disease worldwide (Eat the street food in Delhi once and you’ll see why.)
[NK note: Infectious disease, gastrointestinal, or cardiovascular - choose your burden]

For the middle-class, using government-run hospitals is not preferred. And since it’s increasingly common for Indians with white-collar jobs to get health insurance through their employer they prefer to use this cover at private hospitals.
The annual cost of an employer-funded health insurance plan for an employee ranges from $50-250 depending on their age and the ages of their dependents. However, health insurance only covers in-patient care. That means you can only use it when you have a serious procedure for a critical illness. (aka catastrophic care)
So all the other expenses like urgent care, specialist visits, lab tests, and medicines are all paid Out of Pocket. [NK note: ayyy] A standard blood test is about $10. A specialist visit can range anywhere from $10 to $30. Over the course of a year, a typical Indian family will end up spending about $150 USD on out-patient care.
Where do you think things are working particularly well for India?
Amrit:
1) Doctors often use Whatsapp to speak with patients and issue prescriptions. It’s common for virtual consults to happen on Google Meets. They have tons of flexibility around tools which makes it easier to scale care.
2) Because of the population size, hospitals in major cities in India need to be built with volume in mind. Hospitals like Narayana Health are particularly well known for their ability to do high volumes of complex surgeries like cardiac cases and organ transplants. Another chain, Dr. Agarwals, is known for its low cost cataract surgeries, charging only $300 per eye. A U.S. hospital charges around $4,000 per eye.
[NK note: A little gruesome, but it’s pretty crazy to watch videos of some of these specialized surgery centers in India like the Aravind Clinic. Here’s one that shows a cataract surgery in 3 minutes because they’re essentially parallel processing patients on tables right next to each other, allowing them to do 13-15 surgeries in an hour.]
3) A new class of startups has emerged, focused on attacking chronic conditions, using the playbooks that have worked in the West. (See Beato following Livongo) Because of the relaxed legal frameworks in healthcare, Indian startups are able to quickly test what works and scale those services to millions of Indian patients.
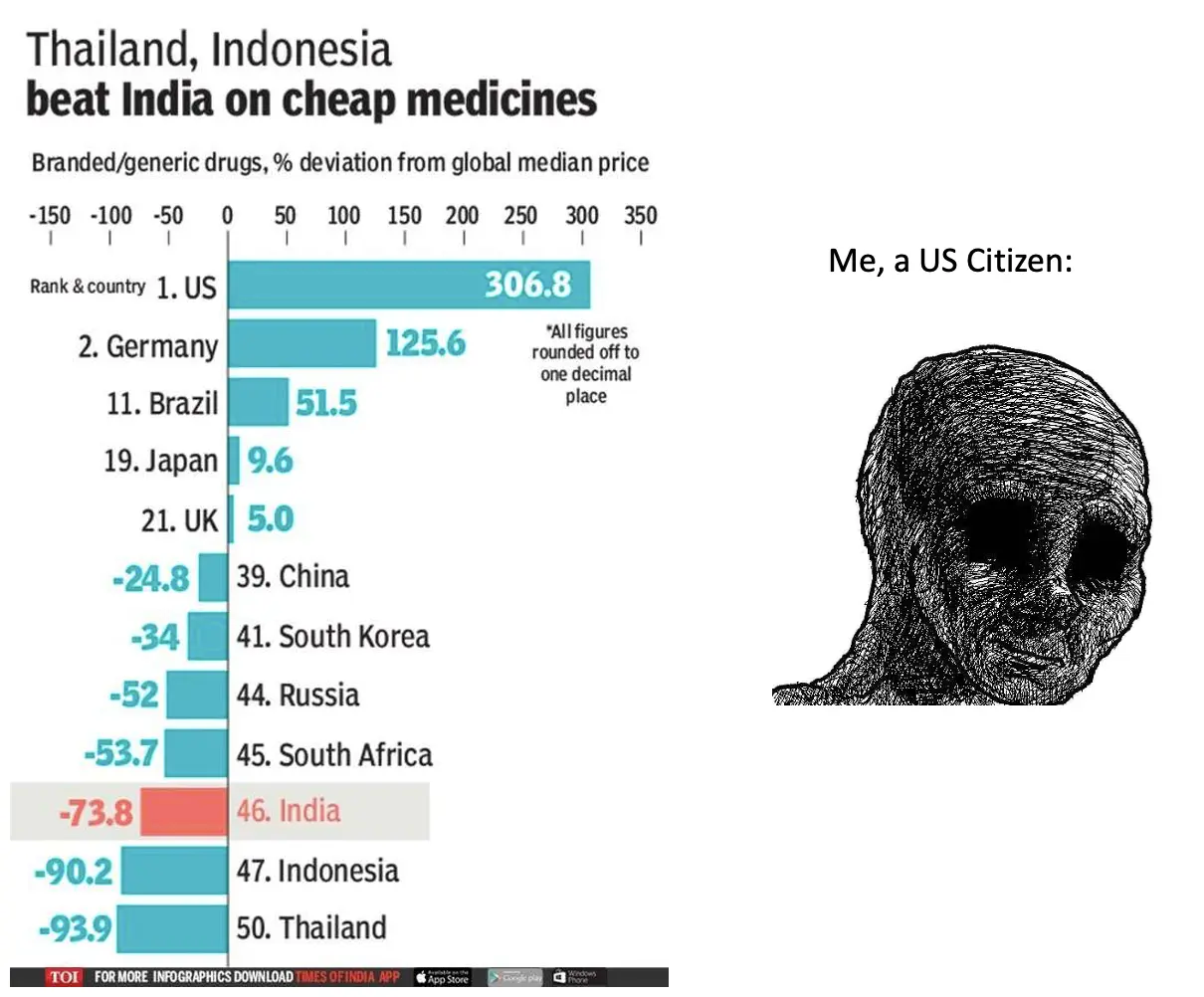
4) India is the world’s largest exporter of generic drugs, so medicines can be found relatively inexpensively here.
There's been a lot of talk in the last few years about the PM-JAY system. What is it and how has the rollout of it been?
Amrit: PM-JAY (akin to Medicaid) is a health insurance plan launched by the Government of India in September 2018. The plan aims to provide financial protection to poor and vulnerable families for secondary and tertiary care.
Under this plan, eligible families are entitled to receive health insurance coverage of up to 500k rupees (approximately $6,700) per family per year. The average overnight hospital visit costs about 75k rupees (approximately $900) so this is actually a good amount of coverage.
The rollout of PM-JAY has been significant, with over 400 million members enrolled in the plan since its inception. It covers over 1,600 medical procedures, including cardiac surgeries, joint replacements, and cancer treatments. While it’s a fantastic initiative, the execution has been lacking in some regards.

Though it’s meant to be ‘technology-driven’, with an online portal that allows members to search for nearby empaneled hospitals, many people have faced difficulties accessing the services due to the shortage of healthcare professionals and inadequate infrastructure. We expect that this will get better as the program matures.
[NK note: Every government has to roll out a technically challenged health insurance enrollment portal, it’s a canon event]
What has the role of the employer traditionally been in the Indian healthcare ecosystem? Has that been changing/why?
Amrit: In the 80s and 90s multinational American and European companies came to India en masse to set up corporate offices, call centers, and IT operations. They offered health insurance as a standard employee benefit.
To compete for talent, Indian companies started to offer employees health benefits as well. It started with the largest companies (TCS, Infosys) but the domino effect proliferated to smaller companies over the course of a few decades.
[NK note: In tech startups, we call this the “Google cafeteria” effect]
Now any company in a major city in India with at least 50 employees will likely buy a group health insurance policy. Though insurance is not a requirement, white collar workers expect their company to provide some form of health insurance.
In just a few decades, 200m people have received health insurance in India, just shy of 20% of the population. The market is growing fast! Every year, it expands by 30%, with more employers opting for some form of health insurance.

Nearly 95% of employers work with brokers to procure quotes from insurance companies, as is common in the US. Self-insured employers are very rare. Health insurance makes up just 2% of total employee salary on average, so it doesn’t make sense for employers to try to set up their own plans (unless the company is really sizable).
What does software usage look like in the Indian healthcare system? How are mobile phones used?
Amrit: The healthcare system in India predominantly runs on mobile phones and paper, though basic business management software is used in large hospitals. Data related to health and medical information is not specifically regulated, so there’s no requirement to uniquely treat health data or digitize it.
It’s now common for doctors to list their services on care aggregator platforms like 1MG, Practo, and Lybrate. These aggregators (think Amazon for doctors) have also built back-office tools for doctors to more easily manage their workflow, scheduling appointments and issuing scripts.
Again, for the most part, no specific software is used. Whatsapp is fairly popular for video consults, chat-based consults, sending a prescription, etc.

[NK note: Interesting that scheduling ends up being a wedge into something that looks more like a one stop shop e-commerce experience.]
Are EHRs a chokepoint there like in the US?
Amrit: Crazy enough, many small and medium hospitals in India still operate on paper-based forms with physical filing systems. These facilities have no way of analyzing longitudinal health data effectively and it’s extremely difficult to retrieve older patient notes.
Larger hospitals do use software, but it’s usually administrative software for scheduling, record keeping, and billing. The receptionists use the software, but not to the doctors themselves.
[NK note: here’s a fun “would you rather” - have your health information fully digitized so your doctor can pull it easily, or be able to self-schedule any of your appointments]
What is the role of ayurvedic practitioners vs. traditional "western" medicine?
Amrit: I don’t know enough about US healthcare, so my understanding of the difference is a bit limited. Here is my understanding:
Access to Physicians is limited in India. As of 2020, India had only 0.8 physicians per 1,000 population, while the United States had 2.6 physicians per 1,000 population.
As a result, there are 1 million+ ayurvedic practitioners in India who have BAMS or MBBS degrees (focus on homeopathy and ayurveda). These people serve the majority of primary care level health issues for the Indian population.
Many Indians treat Ayurveda as a “first line of defense”. For a basic cough and cold, a person might see their local BAMS doctor and pay around $5 for a 10 minute consultation. That doctor would likely suggest a natural approach: things like OTC cough drops, hot tea, and sleep. If the condition worsens, the person would concede to a more expensive visit with an MD aka an allopathy-trained doctor.
[NK note: The tea itself in the US would be $5. I think more use of holistic medicine is great, but also does raise the question of whether people know to escalate to allopathy when it’s necessary. The ayurvedic doctor isn’t exactly incentivized to refer out.]
How does delivery of care work in rural areas in India? Rural health is a problem we struggle a lot with in the US, maybe there are some lessons we can take away.
Amrit:
- Health worker training: Programs have been implemented to train people as nurse practitioners within a short period of time and then to send them to rural areas where care is needed. A well known program called Accredited Social Health Activists (ASHA) has trained more than 1 million people so far.
- Health insurance coverage: Government-sponsored health insurance plans, like Ayushman Bharat, have increased access to affordable healthcare for rural populations, reducing out-of-pocket expenses and financial burden. This is like the Medicaid of India, and covers a massive portion of the population. The bottom 500 million people qualify and most of these people live in rural areas.
- Integration of traditional medicine: Integrating AYUSH (a government initiative), such as Ayurveda and Yoga, with allopathic medicine provides a more holistic approach to healthcare in rural areas.
How do physicians/providers get paid? Is it fee-for-service? Is value-based care a concept and has it gotten any adoption?
Amrit: In India, physicians' payment structures are almost entirely fee for service. In private practice or clinics, physicians charge patients directly for consultations and procedures. In hospital settings, insurance plans are commonly claimed against.
In India it's very common to see the results of the misaligned incentives that stem from fee-for-service models. The focus on volume over outcomes regularly leads to unnecessary tests and treatments, compromising patient health. See the suspicious insanely high rates of C-section births and the common practice of unnecessary stenting.

Value-based care is not a prevalent payment model yet in India. However, some points to ponder:
- The National Health Authority of India will incentivise hospitals for providing value-based services for any government run plans.
- Five performance indicators considered: satisfaction, re-admission, expenditure, grievances, health improvement.
Because most hospitals use disparate software tools and much of record-keeping is done on paper, it will be really difficult to capture this data at scale. However, these incentives may force hospitals to standardize their data frameworks.
[NK note: For countries that are basically rolling out insurance for the first time now, would it make sense to try and go straight to value-based care instead of incentivizing fee-for-service? Maybe in this case it’s logistically impossible without EHR penetration, but it could also be the incentive to start digitizing more processes, idk]
Bonus: If there were one food concept we should bring from India to the US, or US to india, what do you think it should be. Could be a restaurant, fast casual, consumer packaged good, etc.
Amrit: I’d love to see a Chipotle in India. I think it’s a no-brainer. The Indian taste-buds are primed for Mexican food and it’s hard to find a decent burrito anywhere in Mumbai. Taco Bell has been rapidly expanding here already so there are early signs Mexican food is here to stay.
[NK note: My idea, micro dosa stands in the US. There are so many dank dosa stands in India that need very little physical footprint and make an excellent snack that’s pretty portable.]

Thinkboi out,
Nikhil aka. "a super ABCD, aka. EFGH”
Twitter: @nikillinit
Other posts: outofpocket.health/posts
---
If you’re enjoying the newsletter, do me a solid and shoot this over to a friend or healthcare slack channel and tell them to sign up. The line between unemployment and founder of a startup is traction and whether your parents believe you have a job.
Quick Interlude - NEW COURSE ON FHIR! KNOWLEDGEFEST APPS DUE SOON!
See All Courses →So...what actually is FHIR? I get this question a lot, but there's never really enough time to explain it and also I would just mumble "technical standard" and walk away.
So we decided to do a standalone free FHIR 101 course in partnership with Redox! Over 3 days in August we'll go over the spec itself, how it differs from other healthcare information standards, and practical tips to build with it.
I wanted to call it FHIR fest but it got nixed. You can sign up for it here, it's FREE and it's 8/25-8/27.

And a reminder that Knowledgefest apps are due this week. If you want to be in a room with the best ops people in healthcare, you should apply like TODAY.
We sell this conference out every year - all workshops, learn how people are building and scaling in healthcare, application based so we only take the best. We have people from Commure, Clarity Pediatrics, Pomelo, and Waymark already coming, join the squad.

Get Out-Of-Pocket in your email


